


















 53 / 64
53 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 6, November/December 2020
AFRICA
333
In normal physiology, the vectors at the end of depolarisation
and the beginning of repolarisation neutralise each other. On
the ECG, this manifests as a J point (start of ST-segment),
which is not deviated from the isoelectric line.
3
This balance of
charge is maintained by Na
+
/K
+
ATPase channels, which are
dependent on glucose. In coronary artery occlusion, the lack
of glucose supply causes malfunctioning of these ion-gated
channels, resulting in an imbalance of electrical charge across
the myocardial cell membrane. This imbalance in electrical
charge manifests as ST-segment deviation. Transmural ischaemia
leads to ST-segment elevation in leads overlying the ischaemia,
whereas sub-endocardial ischaemia can manifest as ST-segment
depression or T-wave inversion.
4
However, in some cases,
ischaemia can be electrocardiographically silent.
5
ST-segment depression can represent reciprocal changes of
ST-segment elevation recorded by leads opposite those overlying
the acute infarction (Table 1). Because the standard 12-lead
ECG does not include leads that overlie the posterior aspect of
the heart, ST-segment depression in the anterior leads should
prompt the acquisition of posterior leads (V7, V8 and V9) to
rule out posterior ST-segment elevation (Fig. 4).
6,7
ST-segment
elevation in the posterior leads confirms the diagnosis of
posterior STEMI. If no ST-segment elevation is recorded in the
posterior leads, non-ST-segment elevation myocardial infarction
(NSTEMI) (Fig. 5) or pulmonary embolism (PE) (Fig. 6) should
be considered as alternative diagnoses.
Acute posterior STEMI can be accompanied with inferior
STEMI if the culprit lesion is proximal to the posterior
A
LAO CAU
RAO CAU
B
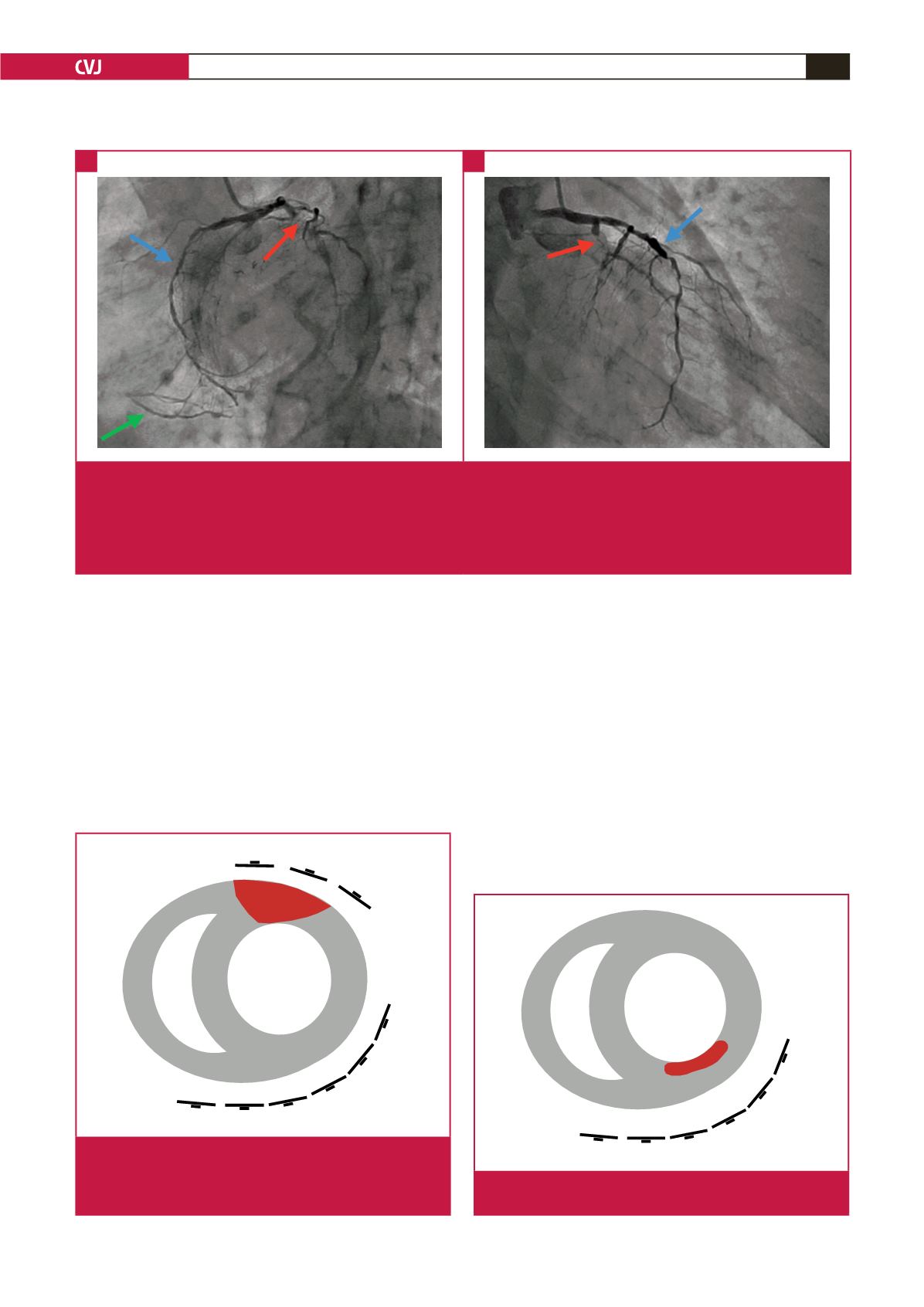
Fig. 3.
A. Left anterior oblique (LAO) caudal view demonstrated extensive coronary artery disease. The proximal left circumflex
artery (LCx) was totally occluded (culprit lesion) (red arrow), and the left anterior descending artery (LAD) was severely
diseased (blue arrow). The posterior descending artery (PDA) filled competitively from left to right collaterals (green arrow).
B. The culprit lesion was the proximal occlusion of the left circumflex artery (LCx), as shown in this right anterior oblique
(RAO) caudal view (red arrow). There was a long segment of severe disease in the left anterior descending artery (LAD)
(blue arrow).
V1
V2
V3
V4
V5
V6
Fig. 5.
Sub-endocardial ischaemia (NSTEMI) can manifest as
ST-segment depression in the anterior leads.
V1
V2
V3
V4
V5
V6
V7
V8
V9
Fig. 4.
Posterior transmural myocardial infarction (STEMI)
would cause ST-segment elevation in the posterior
leads, which in the anterior leads will manifest as
ST-segment depression (reciprocal changes).
A
B