


















 6 / 60
6 / 60

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 32, No 2, March/April 2021
60
AFRICA
The AHRE burden, which takes into account the number and
duration of episodes, may be a better description compared to the
longest AHRE alone. The absolute burden required to increase
thromboembolic risk remains unclear. A re-analysis of ASSERT
only demonstrated an increased risk of stroke for AHREs of
longer than 24 hours.
8
The role of anticoagulation in the management of AHREs
is still being investigated in randomised, controlled trials. The
temporal relationship between AHRE and stroke risk also
remains unclear. The finding from the ASSERT and TRENDS
(The Relationship between daily atrial tachyarrthymia burdEN
from Implantable device Diagnostics and Stroke risk) trials, that
only a quarter to a half of patients sustained an AHRE within
one month of the stroke, suggests that AHREs may be a marker
of increased risk and not directly causative.
9,10
Until these answers are obtained from ongoing trials, individual
practice is likely to vary and be guided by expert opinion. The
2020 European Society of Cardiology atrial fibrillation guidelines
recommend a complete cardiovascular examination with an ECG,
including risk-factor management and thromboembolic risk
assessment, using the CHA
2
DS
2
VASc [Congestive heart failure,
Hypertension, Age ≥ 75 years, Diabetes mellitus, Stroke, Vascular
disease, Age 65-74 years, Sex category (female)] score.
2
Clinicians need to monitor for clinical AF and an increase in
burden of AHREs. The most important management decision
is whether to treat with anticoagulants. AHREs are classified
as short (rare), longer (one to 24 hours) and long episodes
(> 24 hours).
2
The guideline recommends consideration for
anticoagulation in patients with CHA
2
DS
2
VASc scores ≥ two
for men and ≥ three for women, and patients with long episodes
of AHREs (≥ 24 hours) and with a high burden of AHREs.
2
Shared decision making is essential. The 2017 EHRA consensus
document on CIED-detected arrythmias recommends initiating
lifelong anticoagulation therapy if the episode was longer than
5.5 hours, based on the patient’s CHA
2
DS
2
VASc score (≥ one, male
patient; ≥ two, female patients).
3
In summary, AHREs have emerged as an important
cardiovascular condition that is likely a precursor to AF.
Recognising this entity as fact needs to trigger the start of a
journey with the patient, which includes regular follow up of the
Atrial
marker channel
Atrial
EGM: A tip to ring
Ventricular EGM: RV tip to ring
Ventricular marker channel
Atrial marker channel
Atrial EGM: A tip to ring
Ventricular EGM: RV tip to ring
Ventricular marker channel
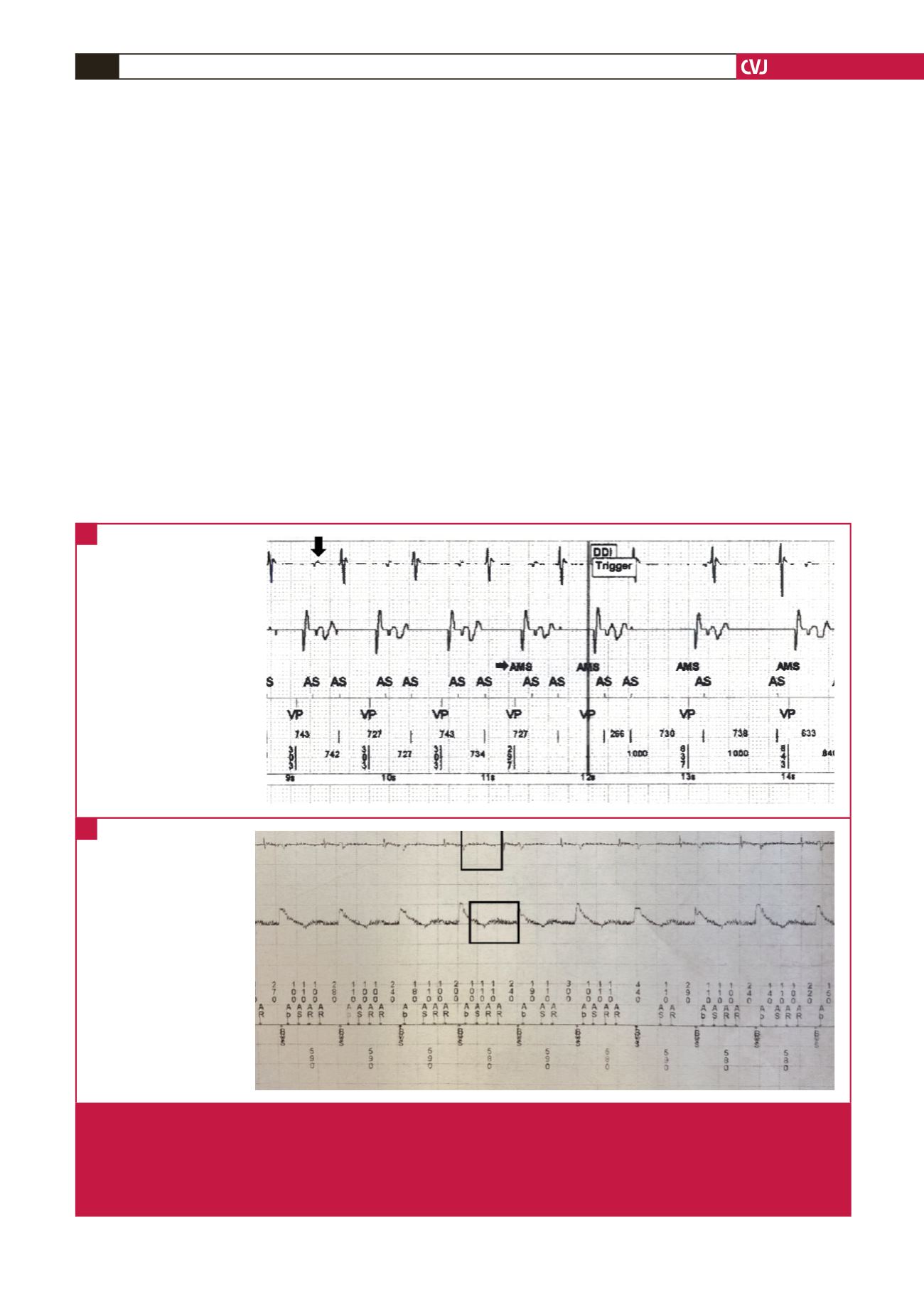
Fig. 2.
Intracardiac EGMs and marker channels depicting examples of AHREs consistent with oversensing. A. Far-field R-wave
oversensing. The arrow indicates far-field R-wave sensing in the atrial channel (atrial EGM), which results in double counting
of the atrial rate. P waves are annotated as AS or atrial sensed, and paced QRS complexes as VP or ventricular paced in
the marker channel. B. Oversensing due to electromagnetic interference. The boxes indicate high-frequency electromagnetic
noise in both the atrial and ventricular channels. Note the marker channel, which shows very rapid non-physiological inter-
vals (annotated as AS and AR or atrial refractory).
A
B