CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 4, July/August 2010
AFRICA
215
erty of compliance in diastole. Ischaemia and disease processes
leading to increased afterload affect diastole by impairment of
the active rate of relaxation.
Left ventricular diastolic dysfunction and heart
failure
The prevalence as well as overall significance of diastolic heart
failure has become distinctly apparent. Diastolic heart failure
was originally reported in 1937 when Fishberg referred to it as
‘hypodiastolic failure’, a form of cardiac insufficiency secondary
to inadequate filling of the left ventricle during diastole.
15
A half
a century later, Kessler became the first to discuss the clinical
syndrome of diastolic heart failure.
16
Over the years, a number of
landmark publications have guided our current understanding in
diagnosing diastolic heart failure.
Recognising the difficulty of non-invasive assessment of the
LV diastolic function, in 2000, Vasan and Levy proposed a clas-
sification scheme for diagnosis of diastolic heart failure in the
hope of reducing the difficulty of diagnosis of this rather preva-
lent pathology.
17
According to the degree of diagnostic certainty,
patients were partitioned into possible, probable, or definite
diastolic heart failure. While keeping the need for evidence
of heart failure for all categories, the diagnosis of probable or
definite diastolic heart failure required evidence of normal left
ventricular systolic function within three days of the initial heart
failure event. Most importantly it was argued that ‘evidence
of abnormal LV relaxation, filling, diastolic distensibility, or
diastolic stiffness’ is required for a definite diagnosis of diastolic
heart failure.
More recently, Zile and colleagues have published several
prospective studies, concluding that the diagnosis of diasto-
lic heart failure does not require objective recording of left
ventricular diastolic dysfunction but only documentation of
preserved systolic function. In two separate studies utilising
both Doppler echocardiography and cardiac catheterisation, the
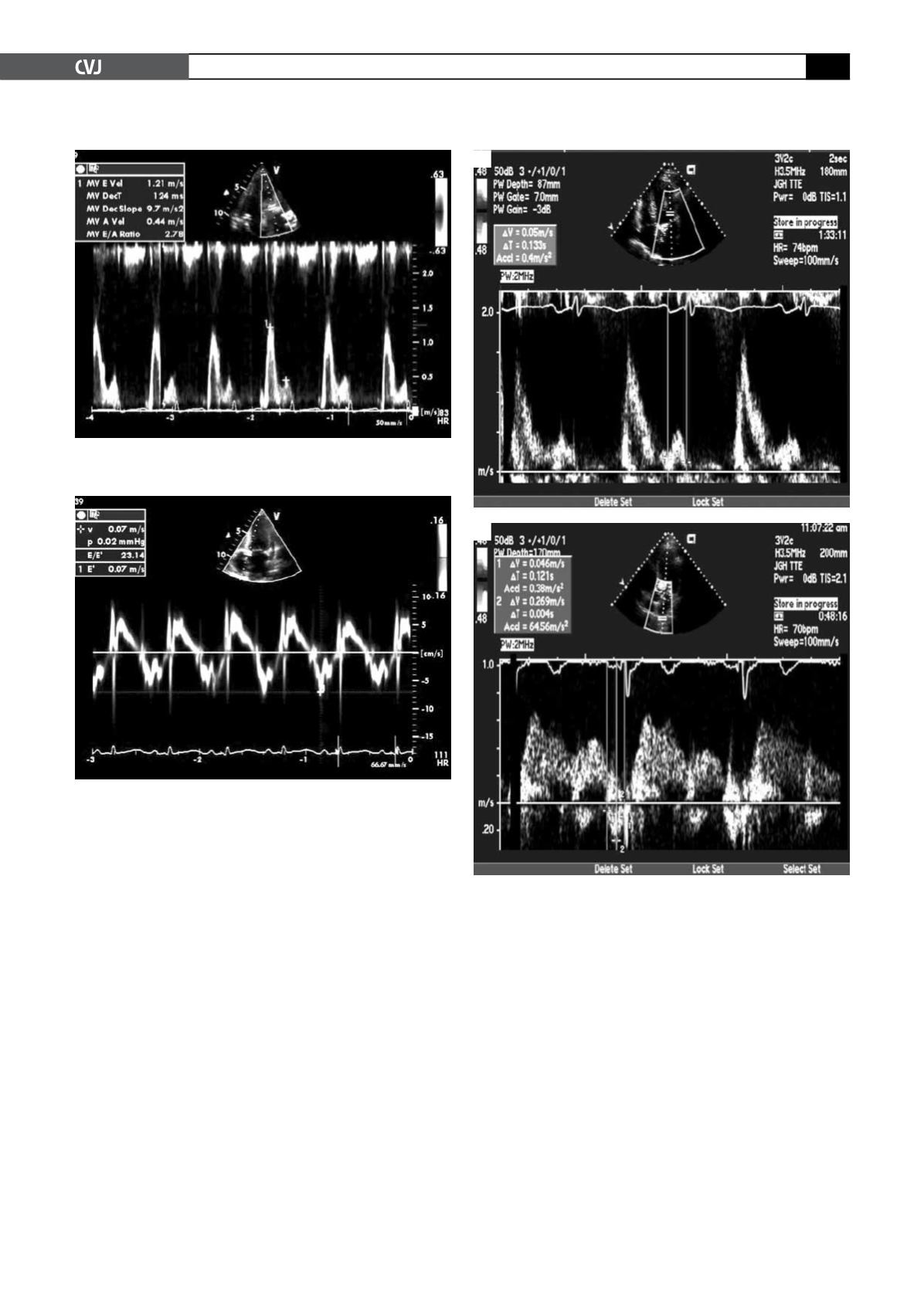
Fig. 5. Stage III diastolic dysfunction: restrictive stage of
diastolic dysfunction: E/A ratio
>
2.0, DT
<
160, IVRT
<
70.
Fig. 6. Doppler tissue imaging (DTI): E¢
<
7 indicates
restrictive filling pattern. The E/E¢
>
15 suggests elevated
PCWP.
Fig. 7. Difference between A duration (mitral) (A) and A
duration of pulmonary vein (B) predicts elevated LVEDP
or PCWP.
A
B


