CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 4, July/August 2010
AFRICA
221
Case Reports
A halo in the heart during coronary angiography:
calcified left ventricular aneurysm with thrombus
formation
H FOTBOLCU, K OZDEN, C SENGUL, D DUMAN, İ DİNDAR
Summary
A 74-year-old man presented with chest pain and dyspnoea
at the cardiology outpatient clinic. His past medical history
included an anterior myocardial infarction in 2008. In the
coronary angiogram, a ‘halo image’ was seen right after the
injection of the contrast agent, and it corresponded with
the location of the left ventricular aneurysm. A calcified left
ventricular aneurysm with mural thrombus was confirmed
with cardiac MRI and a CT scan.
Keywords:
left ventricle aneurysm, calcification, cardiac MRI,
CT
Submitted 13/10/09, accepted 10/3/10
Cardiovasc J Afr
2010;
21
: 221–222
Case report
A 74-year-old man presented with chest pain and dyspnoea at the
cardiology outpatient clinic. His past medical history included an
anterior myocardial infarction in 2008.
His ECG revealed normal sinus rhythm with poor R-wave
progression in the precordial leads. A transthoracic echocar-
diogram demonstrated a left ventricular aneurysm with a
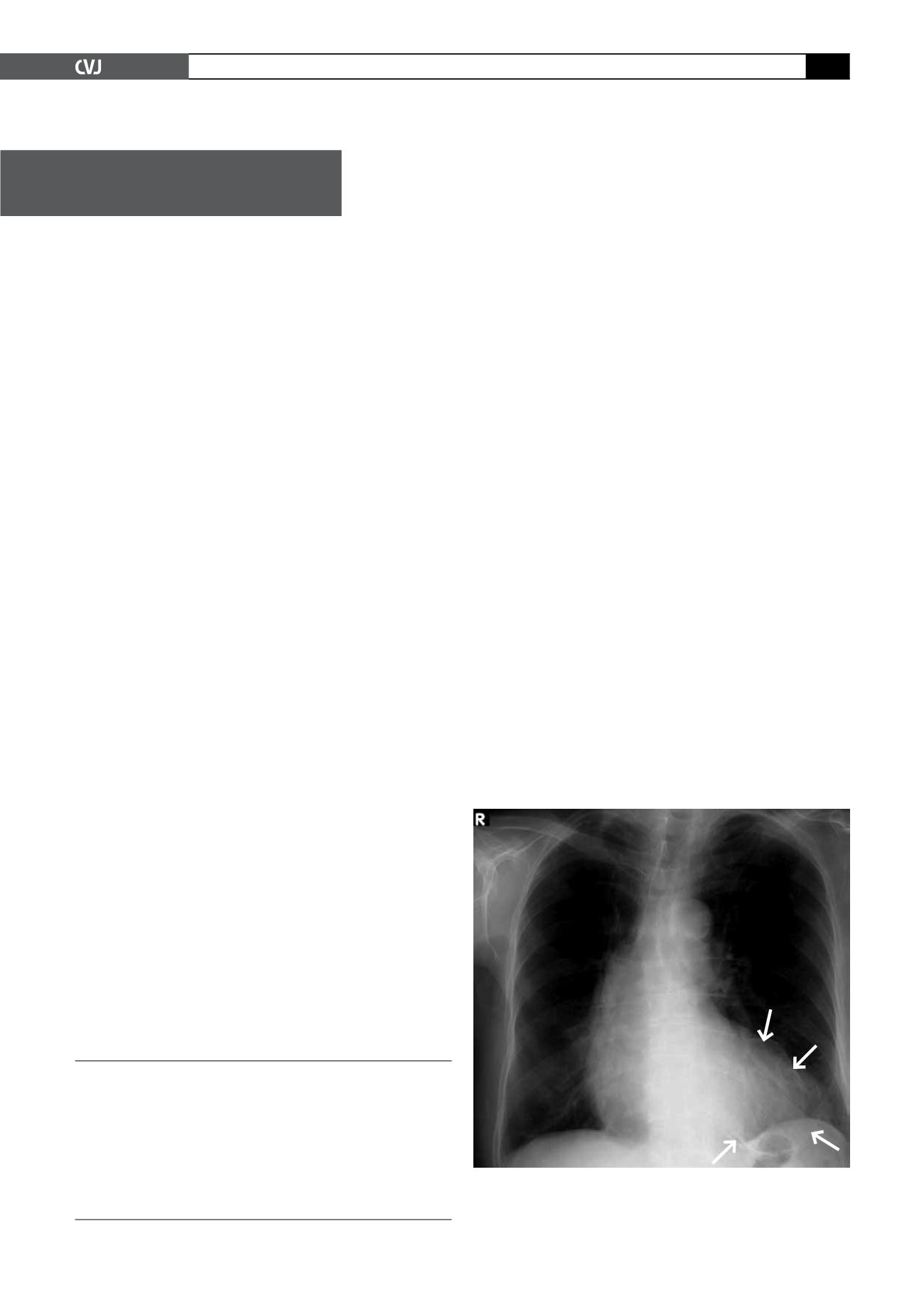
mural thrombus and ejection fraction of 25%. The chest X-ray
showed a peculiar oval calcified image related to a left ventricle
aneurysm (Fig. 1). A nuclear stress test with thalium scintigra-
phy revealed apical mid-anterior, antero-lateral, antero-septum,
infero-septum, inferior and infero-lateral scaring with minimal
peri-infarct ishaemia. In the coronary angiography, a calcified
aneurysm of the anterior wall similar to a huge ‘halo image’ was
seen after the left main coronary artery injection, as well as a
left anterior descending artery occlusion after the first diagonal
branch (Fig. 2). No critical stenosis of the circumflex and right
coronary artery was observed.
Left ventriculography was not performed because of the
possibility of elevated left ventricular end-diastolic pressure,
which might have caused the development of acute pulmonary
oedema. A calcified left ventricular aneurysm with a mural
thrombus was confirmed with cardiac MRI and a CT scan
(Figs 3, 4). The patient was referred for coronary artery bypass
surgery, however he refused to undergo this operation.
Discussion
Left ventricular aneurysm (LVA) is a serious complication
after acute myocardial infarction, and can lead to heart failure.
Despite recent progress in revascularisation techniques, a large
transmural myocardial infarction often results in the formation
of a dyskinetic or akinetic LVA. This is followed by an enlarged
ventricular cavity and abnormal ventricular shape that permits
maximal conversionof tension generated by the myocardium into
cavity pressure, and then congestive heart failure, arrhythmia and
thrombogenesis.
1
Curvilinear calcification at the left ventricular apex strongly
suggested the presence of an aneurysm. The distribution of this
Goztepe Medical Park Hospital, Division of Cardiology,
Istanbul, Turkey
HAKAN FOTBOLCU, MD,
KİVİLCİM OZDEN, MD
CİHAN SENGUL, MD
İSMET DİNDAR, MD
Haydarpaşa Numune Training and Research Hospital,
Department of Cardiology, Istanbul, Turkey
DURSUN DUMAN, MD
Fig. 1. Thoracic X-ray showing an enlarged heart, and
an oval-shaped calcified structure (arrows) related to a
calcified antero-apical left ventricular aneurysm.


