CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 4, May 2012
e4
AFRICA
Case report
A 65-year-old man with a history of stable angina was
admitted to our institution for an elective CABG operation.
He had hypertension, hypercholesterolaemia, diabetes mellitus
controlled with oral medication and a smoking history of 50
years. The patient had no neurological complaints. The central
nervous system and cardiovascular system were normal.
On his chest X-ray, the aortic arch seemed dilated and
mildly calcified (Fig. 1). Coronary angiography revealed
triple-vessel disease with a left main coronary artery lesion
of 60%. In our protocol, all patients scheduled for CABG
operations are simultaneously scheduled for a pre-operative
TTE examination for evaluation of their valvular and ventricular
functions. In this patient with a mildly enlarged mediastinal
silhouette on chest X-ray, the referring cardiovascular surgeon
involved the echocardiograhy laboratory for a detailed
evaluation of the ascending aorta and aortic arch. TTE
performed at our institution showed minimal aortic regurgitation
with an ejection fraction of 60% and a mobile atheroma
at the aortic arch with minimal aortic dilatation (Fig. 2).
The surgical strategy was modified due to these findings
and the arterial cannulation site was moved to the innominate
artery with a regular two-staged venous cannulation, followed
by a hemi-arcus aorta replacement with a quadruple CABG
(left internal thoracic artery–left anterior descending artery
bypass graft, aorta–diagonal artery–obtuse marginal branch
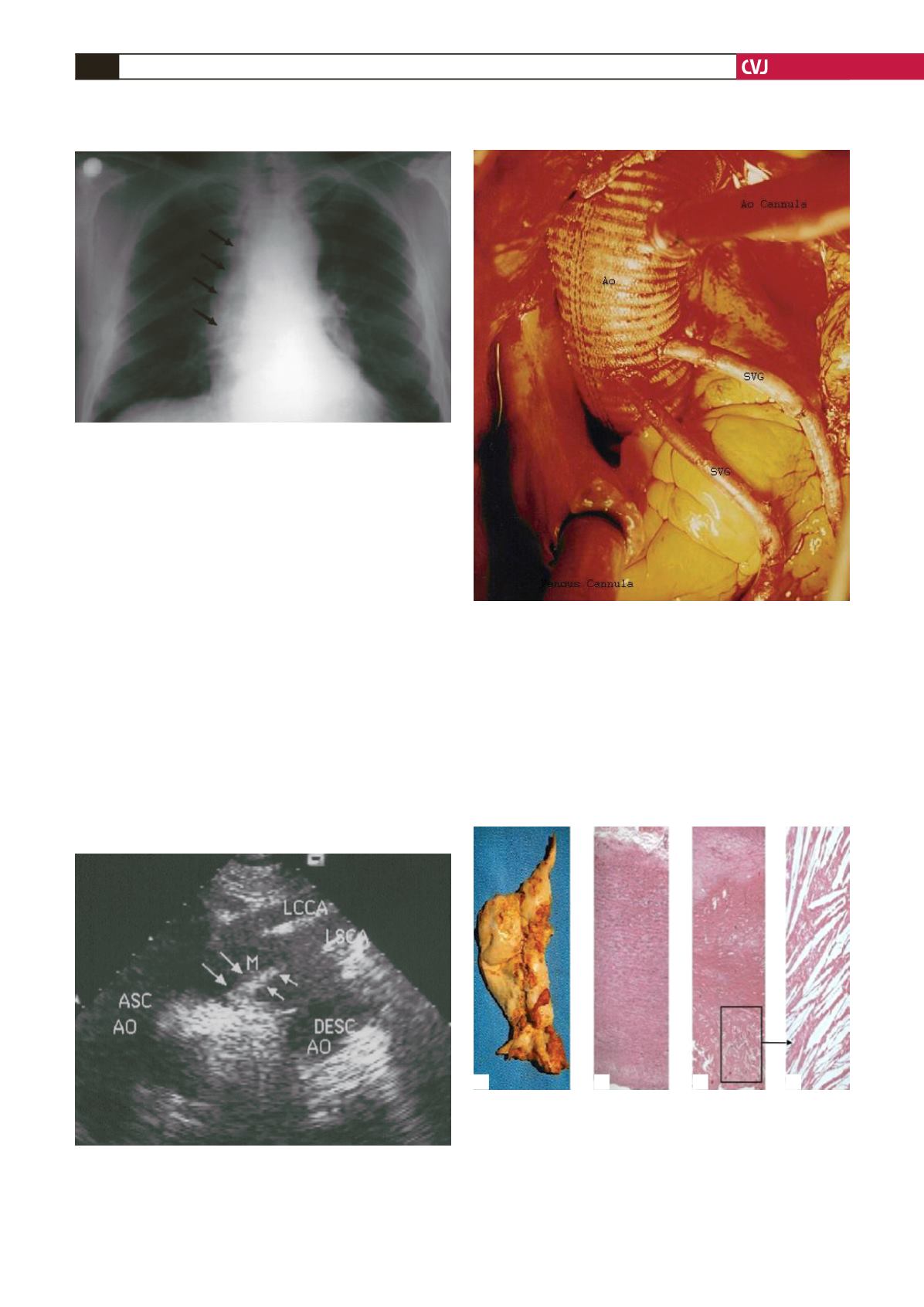
Fig. 1. Pre-operative chest X-ray showing a dilated and
mildly calcified aortic arch (arrows).
Fig. 2. Transthoracic echocardiographic examination
revealing a mobile atheroma at the aortic arch with mini-
mal aortic dilatation. Asc Ao: ascending aorta, LCCA:
left common carotid artery, LSCA: left subclavian artery,
Desc Ao: descending aorta, M: mobile atheroma.
Fig. 3. Photograph taken at the end of the opera-
tion. Hemi-arcus replacement (no: 28 gel-coated dacron
vascular graft) with proximal coronary anastomoses of
the saphenous grafts constructed directly to the aortic
graft. SVG: saphenous vein graft, Ao: dacron vascular
graft.
Fig. 4. Macroscopic and histopathological view of the
aortic arch specimen. A. Excisional aortic specimen with
the mobile atheroma in the aortic arch (arrow) showing
rupture of the tunica intima, atheromas with ulceration,
and a pedunculated thrombus formation attached to the
arterial wall. B, C and D. Histopathological examination of
the specimen showing atherosclerotic intimal changes,
chronic fibrosis and full-thickness degeneration of the
artery.
A
B
C
D


