


















 31 / 67
31 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 2, March 2013
AFRICA
29
of valve disease.
5
Echocardiography (echo) is essential to
confirm the diagnosis and monitor the heart valves to detect
any progression of disease.
7,8
The management of RHD is
complex and requires careful co-ordination. The main goal is
to prevent disease progression and to avoid, or at least delay,
valve surgery. Management of RHD depends on the severity
of disease.
7,8
The need for surgery is determined by the severity
of symptoms, evidence that the heart valves are significantly
damaged, the heart chamber size is distorted and cardiac function
is significantly impaired.
9
To our knowledge, there are no systematically collected data
on newly diagnosed patients with RHD in the Ugandan setting
over the past 30 years. Accordingly, the aim of this study was to
describe the presenting features and complications of patients
who were newly diagnosed with RHD in the Mulago Hospital.
Methods
Institutional ethics approval was obtained from the School of
Medicine Research and Ethics Committee of the College of
Health Sciences, Makerere University. We obtained informed
consent from all patients and informed assent for those unable
to give consent. Patients’ initials and study numbers were put on
the questionnaires instead of full names to ensure confidentiality.
This was a cross-sectional study describing the clinical and
echo features of newly diagnosed RHD patients between June
2011 and January 2012. The study was carried out at Mulago
Hospital, the national referral hospital and Makerere University’s
teaching hospital, located in Kampala, Uganda. Mulago Hospital
handles about 25 patients with newly diagnosed RHD a month at
different clinics, as follows: (1) Uganda Heart Institute located
on ward 1C, Mulago Hospital (in- and out-patient departments)
registers on average 10 newly diagnosed RHD patients per
month;
10
(2) The adult cardiac clinic in the medical out-patient
department (MOPD), Mulago Hospital registers six newly
diagnosed RHD patients per month; (3) The paediatric cardiac
clinic in the MOPD, Mulago Hospital registers about one newly
diagnosed RHD patient per month; (4) The cardiac in-patient
firm (ward 4C), Mulago Hospital admits about eight newly
diagnosed RHD patients per month.
RHD cases were diagnosed using the WHO and United States
National Institutes of Health-recommended echo diagnostic
criteria.
11
Complications of RHD were defined as one or more
of the following: (1) advanced heart failure (NYHA class III/
IV), (2) atrial fibrillation, (3) infective endocarditis (diagnosed
using the modified Duke criteria), (4) pulmonary hypertension,
(5) atrial thrombus, (6) thromboembolic stroke secondary to
atrial fibrillation or infective endocarditis, (7) recurrent ARF
(diagnosed using NIH/WHO criteria).
11
The inclusion criteria
were age five to 65 years of age in newly diagnosed RHD
patients, confirmed by echocardiography (echo) using the
above criteria.
11
Patients with prior echo diagnosis of RHD were
excluded.
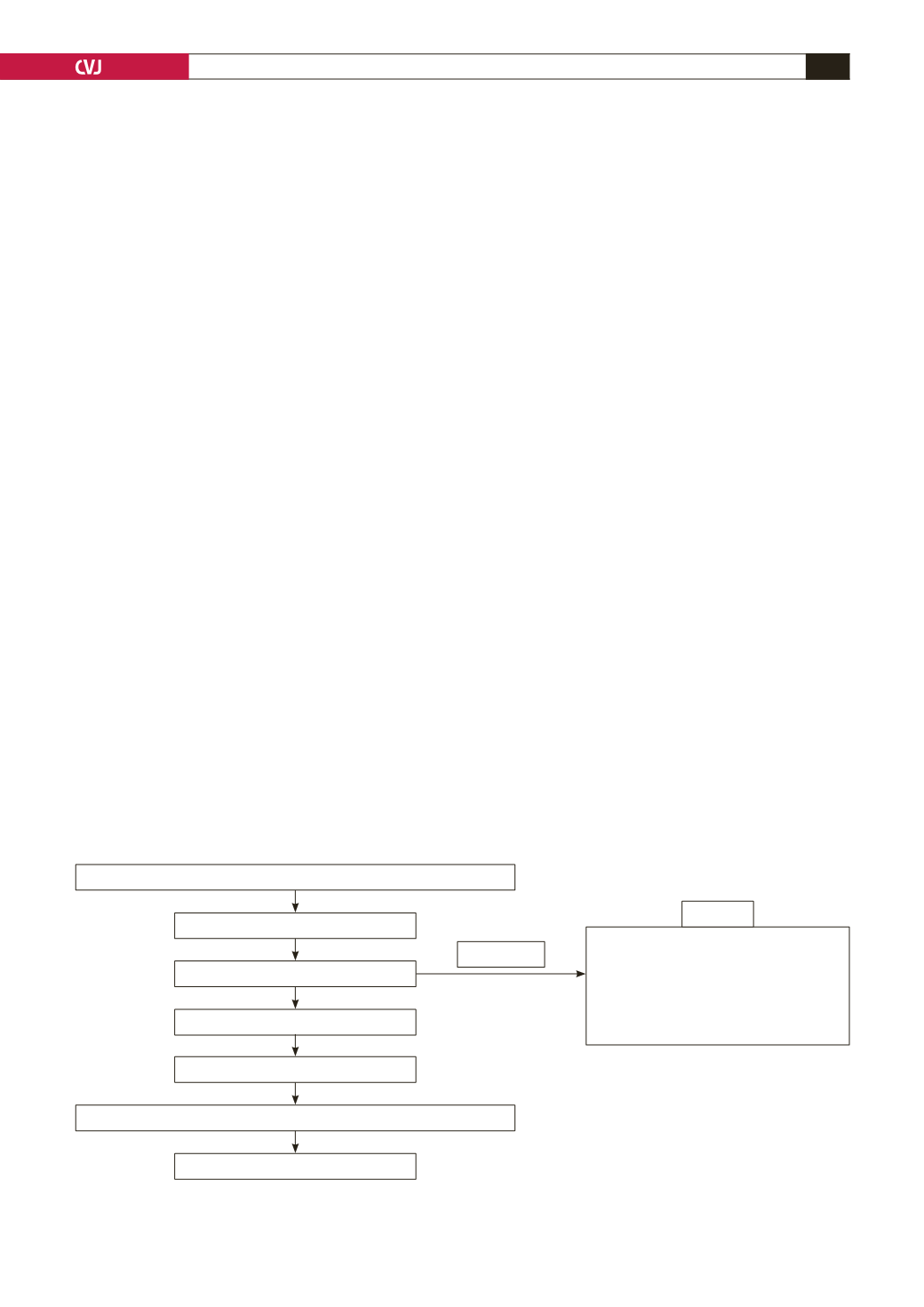
Patients who met the inclusion criteria were consecutively
recruited (Fig. 1) over a period of eight months to reach the
required sample size of 130 patients. Data on demographic
variables (age, gender, tribe, residence, occupation, income
level, education level) and clinical variables (history, physical
examination, laboratory investigation variables, rest ECG, echo)
were recorded on a standardised questionnaire.
Transthoracic echocardiography (TTE)
A commercially available cardiac ultrasound machine, Vivid
7 Dimension, GE Medical Systems (Horten, Norway) with
dedicated capabilities for cardiac evaluation, was used to acquire
the images. Image acquisition was performed according to the
ASE guidelines.
12
Briefly, transthoracic echocardiograms were
performed with the subjects at rest in the left lateral decubitus
position by the principle investigator, under supervision of an
experienced cardiologist. The recorded images were reviewed
by two independent experienced cardiologists who did not know
the patients. A 3.5-MHz transducer was used for adult (age
>
12 years) two-dimensional, M-mode and Doppler examinations,
and a 5.0–7.5-MHz transducer was used for children (age 5–12
years).
Total (
n
= 26)
Probable/possible RHD (
n
= 13)
Non-RHD (
n
= 13)
Normal echo (
n
= 2)
Congenital heart disease (
n
= 6)
Dilated cardiomyopathy (
n
= 4)
Cor pulmonale (
n
= 1)
Excluded
Patients at the cardiac clinics (UHI, MOPD, 4CC, Paediatric ward)
Suspected RHD (
n
= 156)
Screening echo
No RHD
Confirmed defined RHD (
n
= 130)
Informed consent
Questionnaire + comprehensive echo + ECG + blood investigations
Data analysis (
n
= 130)
Fig. 1. Patients’ flow chart. UHI = Uganda Heart Institute; MOPD = Medical out-patient department; 4C = Ward 4C
cardiology