CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 6, July 2013
AFRICA
221
simplex virus, adenovirus and parvovirus B19 virus were
each detected in 12% of the cases (Fig. 2). Cytomegalovirus
infection was not detected in participants with idiopathic dilated
cardiomyopathy.
A viral prevalence of 90% was found in the heart transplant
recipients as 10 of the 11 cases were positive for at least one
virus as detected by PCR. A mean viral burden of 2.2 viruses per
case was found irrespective of whether patients were classified
as having myocarditis or no myocarditis. The most prevalent
viruses was the enterovirus (50%) and adenovirus (50%),
followed by Epstein-Barr virus (32%) and herpes simplex virus
(25%), with parvovirus B19 (18%) and cytomegalovirus (18%)
being the least common agents (Fig. 2).
Discussion
In this first report of the prevalence ofmyocarditis and cardiotropic
viral infection in African patients with HIV-associated
cardiomyopathy, we show that nearly half of the patients may
have had acute and chronic myocarditis. By contrast, idiopathic
dilated cardiomyopathy was associated with myocarditis in a
quarter of the cases, none of whom had acute disease.
The presence of genomes of cardiotropic viruses was almost
universal inAfrican patientswithHIV-associated cardiomyopathy,
idiopathic dilated cardiomyopathy, and heart transplant
recipients. Furthermore, we observed that participants who were
immunosuppressed by HIV infection or on immunosuppressive
treatment for heart transplantation had double the number of
cardiotropic viruses per case, compared to those with idiopathic
dilated cardiomyopathy (2.2–2.5 viruses per case compared to
1.1 virus per case).
Because heart biopsy and viral genome analysis are rarely
done in many regions of the world, the prevalence of viral
myocarditis in much of Africa, Asia, the Middle East and
South America is unknown.
12
The few endomyocardial biopsy
studies in African patients with cardiomyopathy were conducted
in the pre-HIV era.
13–16
These studies, which did not use
modern techniques of immunohistochemistry and molecular
characterisation of viral genomes, had conflicting findings on
the prevalence of myocarditis.
In the largest endomyocardial biopsy study of 76 South
African patients with idiopathic dilated cardiomyopathy, no
evidence of myocarditis was found, leading to the conclusion
that the cardiac failure of dilated cardiomyopathy was due to an
unknown functional abnormality, such as a toxin or metabolic
defect.
13,14
However, endomyocardial biopsy studies of dilated
and peripartum cardiomyopathy from Kenya revealed that about
half of the patients had evidence of healed myocarditis but no
serological evidence of a previous Coxsackie virus infection or
any other common viral infections.
15,16
The authors concluded
that the myocarditis was due to an inappropriate immunological
reaction to myocardial muscle.
15,16
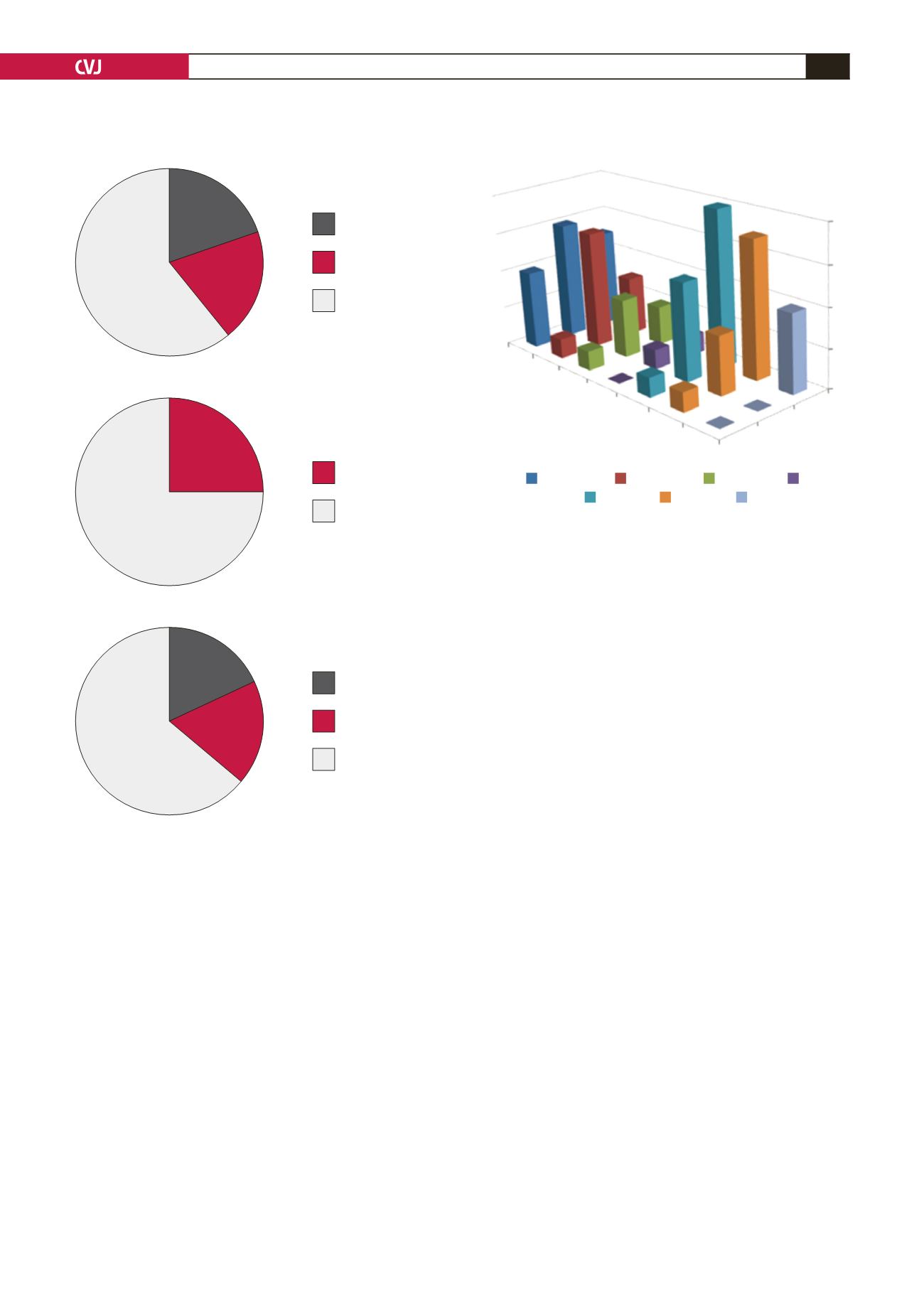
A: HIV-associated cardiomyopathy
B: Idiopathic dilated cardiomyopathy
C: Heart transplant recipients
Fig. 1. Prevalence of myocarditis in HIV-associated
cardiomyopathy (A), idiopathic dilated cardiomyopathy
(B), and heart transplant recipients (C).
Acute myocarditis
Chronic myocarditis
No myocarditis
Chronic myocarditis
No myocarditis
Acute myocarditis
Chronic myocarditis
No myocarditis
Fig. 2. Prevalence of cardiotropic virus infection in
patients with HIV-associated cardiomyopathy (HIVAC),
idiopathic dilated cardiomyopathy (IDCM), and heart
transplant recipients (HTx). Entero, enterovirus; Adeno,
adenovirus; Parvo, parvovirus B19; CMV, cytomegalovi-
rus; EBV, Epstein-Barr virus; HSV, herspes simplex virus;
HIV, human immunodeficiency virus.
Viral presence (%)
Viral infective status of three cohorts using EMB
Cohorts
IDCM
HIVAC
8
6
4
2
0
Entero
Adeno
Parvo
CMV
EBV
HSV
HIV
Entero
Adeno
Parvo
CMV
EBV
HSV
HIV
57.2%
64%
75%
21.4%
18%
21.4%
18%
25%
HTx


