


















 64 / 74
64 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 5, September/October 2014
e6
AFRICA
Postoperative echocardiography and computed tomography
showed a well-functioning prosthetic aortic valve without
regurgitant flow, and a correctly placed stent graft without
endoleak. The patient was discharged two weeks after the
operation. He remained haemodynamically stable until the
discharge. After one month, in an out-patient clinic, the patient
showed good functional recovery.
Discussion
Traumatic injury of the aorta is relatively rare, being reported
in less than 5% of traumatic vascular injuries. However, the
true incidence is likely to be higher, as many victims die prior
to hospitalistion for definitive care.
4
Rupture of the aortic valve
is extremely rare and there are only a few reports to date. Our
patient presented with two different lesions, both from blunt
chest trauma; one was a pseudo-aneurysm at the isthmus of the
aorta and the other a rupture of the aortic valve.
The mechanism leading to damage of the aortic valve in
an accident is suspected to be due to massive increase in intra-
thoracic pressure, leading to an increase in intra-aortic pressure.
When this occurs during the early diastolic phase, the phase
of lower left ventricular pressure, a high pressure difference
could develop across the closed aortic valve. This high pressure
difference causes aortic valve damage.
2,5,6
The descending aorta is attached to the chest wall, whereas
the heart and great vessels are relatively mobile. Therefore,
a traumatic injury of the aorta more frequently involves the
descending rather than the ascending aorta.
2,7
Traditional views
have been that sudden deceleration causes a tear at the junction
between the fixed and mobile portions of the aorta, usually at
the aortic isthmus distal to the origin of the left subclavian artery
(ligamentum arteriosum).
8
Injury of the ascending aorta caused by chest wall trauma
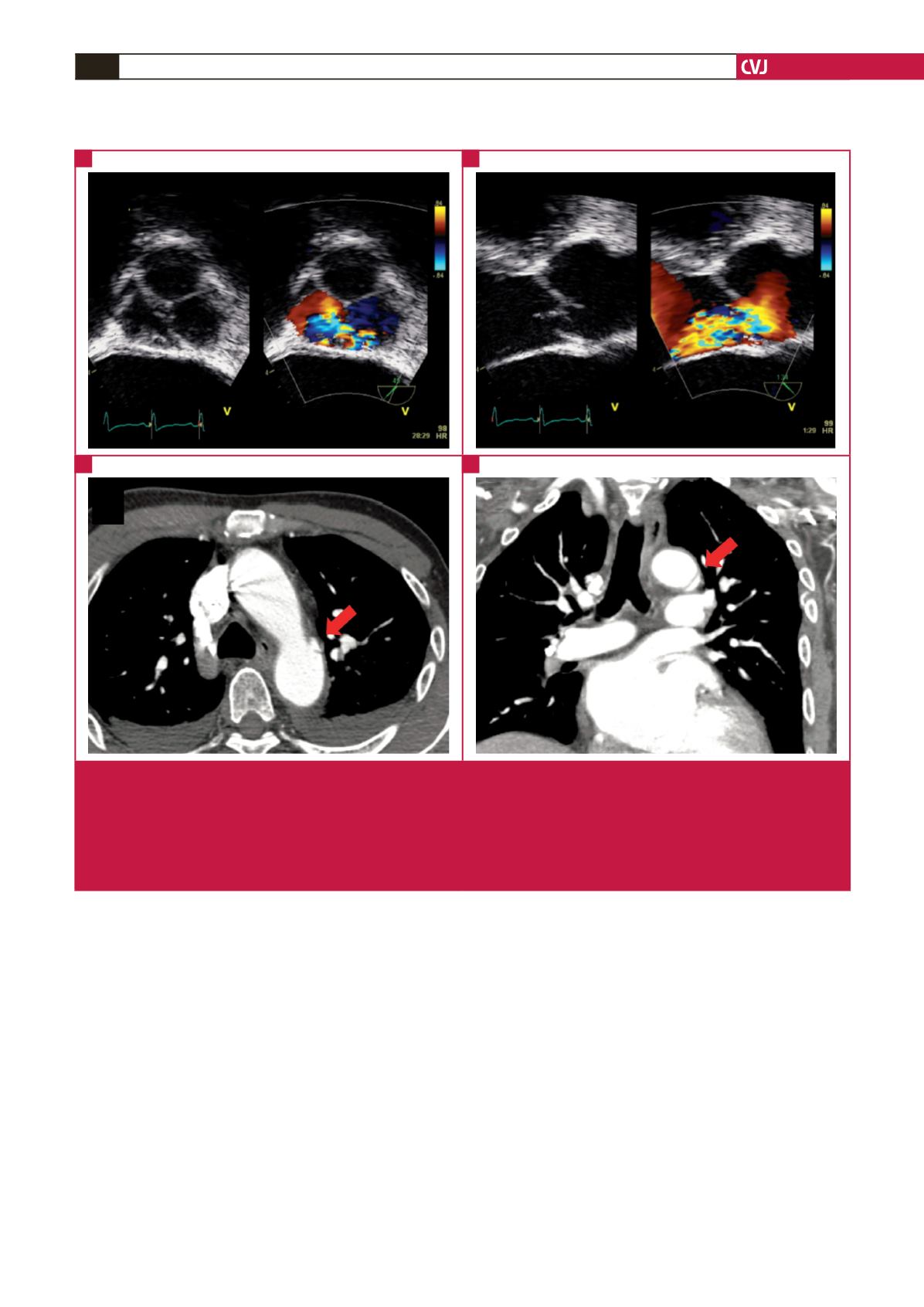
Fig. 1.
Aortic regurgitation shown in transoesophageal echocardiography and pseudo-aneurysm seen in computed tomography.
(A) In the short-axis view, a tear of the non-coronary cusp was suspected, and in the short-axis view with colour Doppler,
significant severe aortic regurgitation in the region of the non-coronary cusp was seen. (B) A long-axis view revealed rupture
of non-coronary cusp with torn linear tissue, and in the long-axis view with colour Doppler, severe aortic regurgitation with
rupture of the non-coronary cusp was seen. (C) In a post-enhanced axial view, a small pseudo-aneurysm (arrow) in the
aortic isthmus is demonstrated. (D) A coronal reformatted image revealed a small pseudo-aneurysm (arrow) at the level of
the proximal descending thoracic aorta.
A
C
B
D