


















 65 / 74
65 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 5, September/October 2014
AFRICA
e7
is relatively uncommon and usually fatal. The combination of
aortic valve injury and ascending thoracic aorta injury is rare
and there are only a few case reports. Furthermore, there are no
reports of the combination of aortic valve injury and traumatic
pseudo-aneurysm of the aortic isthmus.
The causative mechanism of aortic valve injury is thought
to be different from that of injury of the descending aorta.
2
It
has been reported that post-traumatic aortic valve regurgitation
rather than injury of the descending aorta is often found with
sternal or multiple rib fractures. It has been proposed that the
impact of a fractured sternum could limit displacement of the
heart and ascending aorta during an accident, and this would
prevent traction on the aortic isthmus.
When the thoracic wall is fractured, the movement of the
heart is restricted by the fractured sternum and a force is exerted
on the ascending aorta rather than on the aortic isthmus. This
force would affect the column of blood within the aorta, which
could rupture the ascending aorta or a valve apparatus but
the aortic isthmus would be safe. Therefore, the simultaneous
development of both aortic valve injury and descending thoracic
aorta rupture by external trauma is unlikely to happen.
The exact mechanism of a combination of aortic valve
rupture and traumatic pseudo-aneurysm of the aortic isthmus
is not clearly understood. We propose that the pathophysiology
of aortic injury after blunt chest trauma could be caused by a
variety of mechanisms, not just one.
It is difficult to diagnose aortic regurgitation if a patient has
multiple injuries. Echocardiography, history taking, and physical
examination are helpful to make a diagnosis. However, making
a correct diagnosis my still be challenging since a patient often
presents with multiple traumatic injuries from an accident, such
as chest wall pain, and rib or other bone fractures.
1
Since a
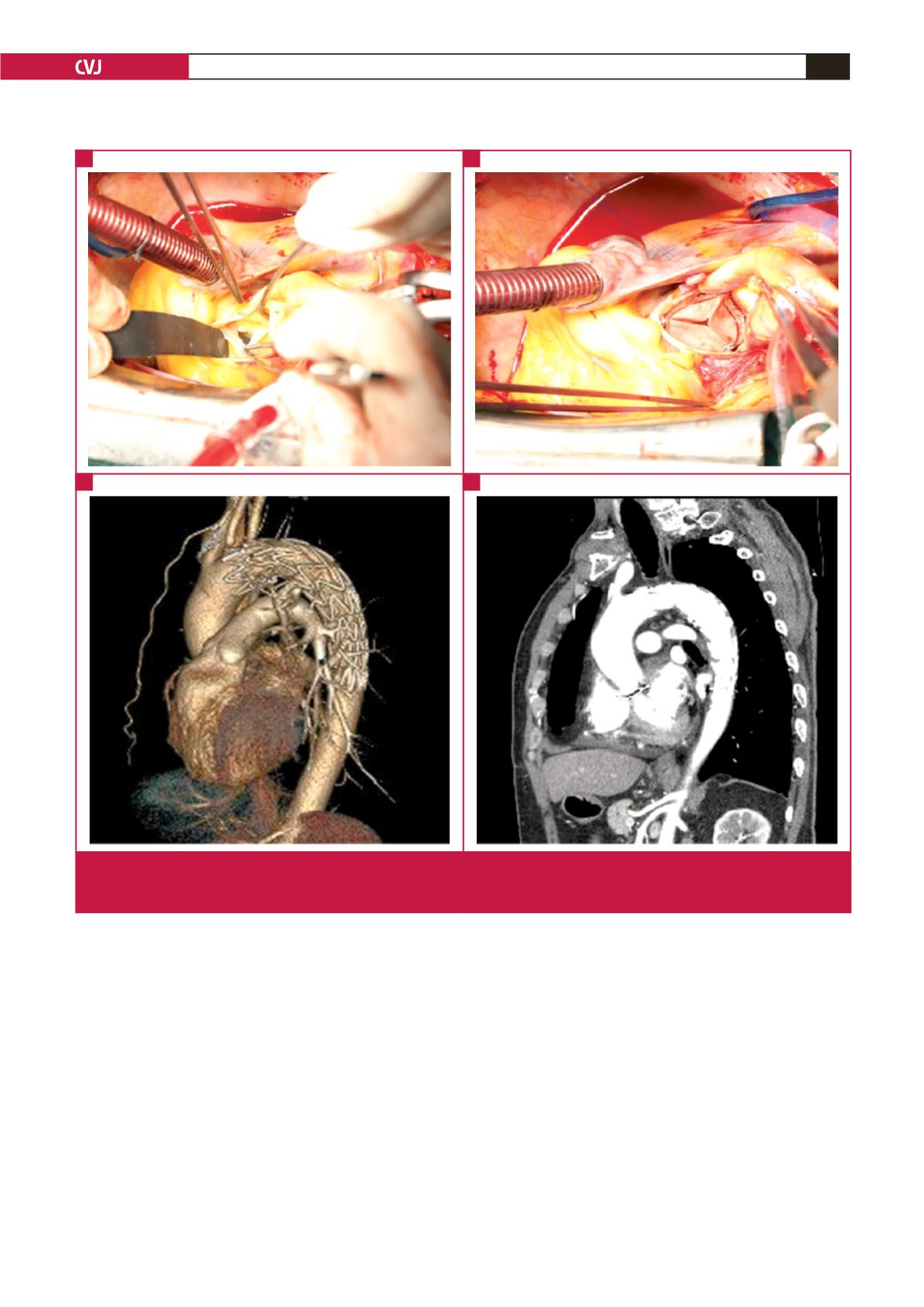
Fig. 2.
Intra-operative photographs of the aortic valve, and CT angiographic findings after implantation of a stent graft. (A) Perforation
of the non-coronary cusp of the aortic valve is seen. (B) The aortic valve was removed and replaced with a bioprosthetic
valve. (C) and (D) The pseudo-aneurysm was not seen after stent graft implantation in reconstructed CT images.
A
C
B
D