


















 36 / 66
36 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 6, November/December 2014
286
AFRICA
showed elevated B-type natriuretic peptide (BNP) levels to be
predictive of AF in patients undergoing CABG.
28,29
The utility
of biomarkers in the setting of AF post cardiac surgery requires
further clarification prior to a recommendation on their use but
preliminary studies certainly show promise for AF prediction
and thromboembolic risk stratification.
With regard to risk-prediction models for the development
of AF, several have been developed and incorporate risk factors,
some of which are mentioned in Table 3. These models have
thus far provided controversial and inconsistent results, which
have limited their widespread adoption. However, studies by
Chua
et al
. and Baker
et al
. demonstrated the CHADS
2
and
CHA
2
DS
2
-VASc scoring systems to be predictive of AF post
cardiac surgery.
30,31
The limitations of these studies are that they
were retrospective in nature, the sample size was small, and the
patient population was heterogeneous. A recent study by Sareh
et al
. showed the CHADS
2
score to be a powerful and convenient
predictor of post-operative AF in a cohort of 2 120 patients.
32
A large, prospective, multicentric trial will provide a definite
answer as to whether the CHADS
2
and the CHA
2
DS
2
-VASc
scoring systems reliably predict post-operative AF. Should this
be proved to be so, physicians will be guided to develop an
effective prophylaxis strategy, including drugs and perhaps even
prophylactic ligation of the left atrial appendage for ‘high-risk’
patients.
Limitations of this study are: it described only post-operative
patients developing AF and an analysis of a control group was
not undertaken. Furthermore, the cohort number was small
relative to other similar studies conducted internationally.
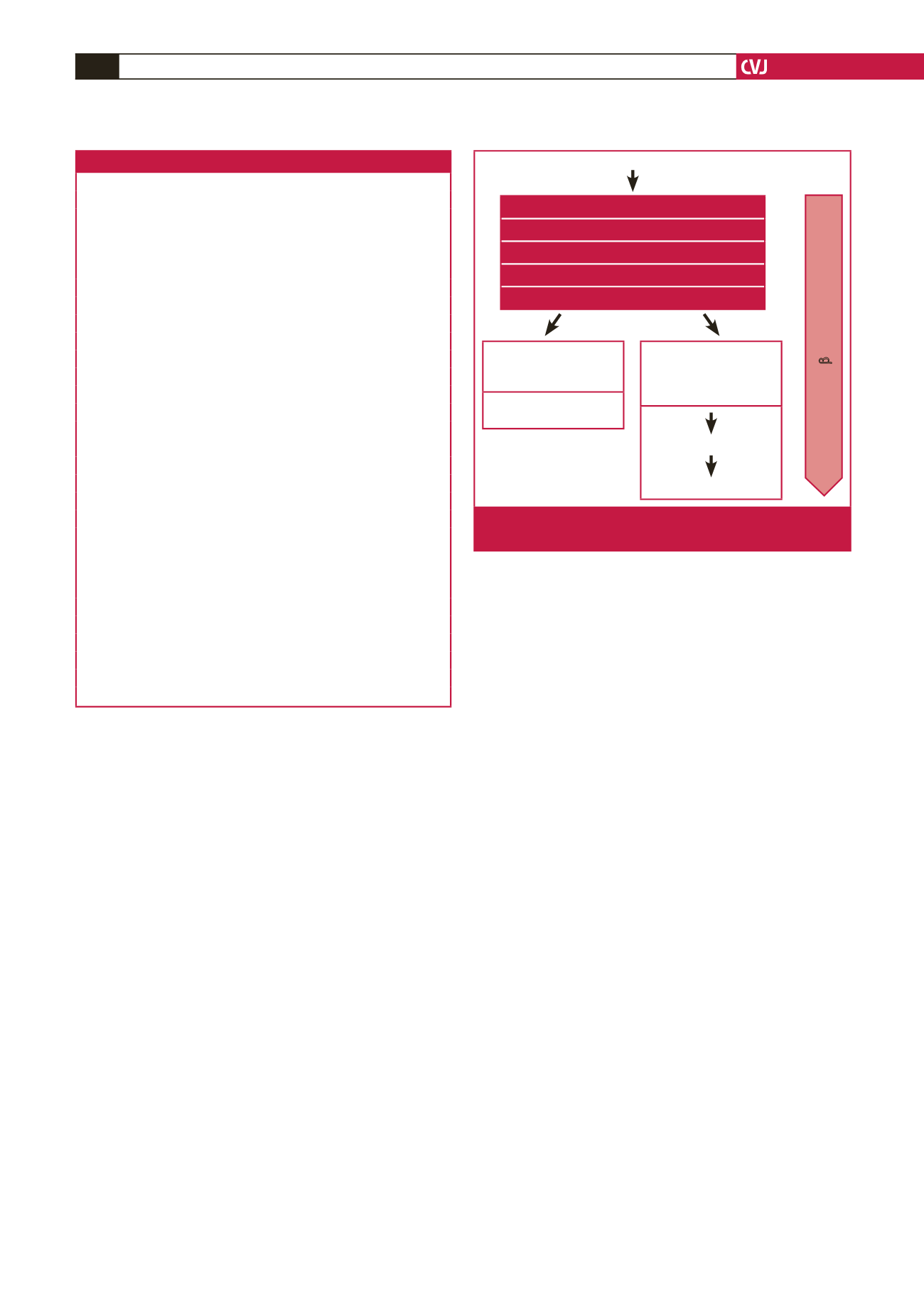
Conclusions
This study serves to add to the growing body of information
regarding
de novo
AF post cardiac surgery and provides some
insight into the problem in developing countries. We propose
a simple algorithm, shown in Fig. 3, for the immediate post-
operative treatment of AF. Experience locally appears to mirror
that of international cardiac surgical units. The aetiopathogenesis
of AF is complex and a plethora of risk factors have been
proposed (Table 3).
33
Use of the CHADS
2
and CHA
2
DS
2
-VASc scoring systems
and cardiac biomarkers as AF predictors appear promising.
Liberal peri-operative
β
-blocker and statin administration is
currently highly recommended. AF prophylaxis for the elderly,
obese Indian male undergoing coronary surgery locally requires
validation. Opportunistic surveillance for AF is advised at
follow-up cardiology visits. Well-designed prospective studies
are required for the better understanding and treatment of this
common post-operative complication locally. The developing
world should concentrate study efforts on LOS and cost
reduction.
References
1. Almassi GH, Schowalter T, Nicolosi AC,
et al
. Atrial fibrillation after
cardiac surgery: a major morbid event?
Ann Surg
1997;
226
: 501–511.
http://dx.doi.org/10.1097/00000658-199710000-00011.2. Dunning J, Treasure T, Versteegh M, Nashef SA, EACTS Audit and
Guidelines Committee. Guidelines on the prevention and manage-
ment of de novo atrial fibrillation after cardiac and thoracic surgery.
Eur J Cardiothorac Surg
2006;
30
: 852–872.
http://dx.doi.org/10.1016/j.ejcts.2006.09.003.
3. Echahidi N, Pibarot P, O’Hara G,
et al.
Mechanisms, prevention, and
Table 3. Risk factors for AF
Pre-operative
Advanced age
Male gender
Hypertension
Previous AF
History of previous cardiac surgery
Congestive heart failure (CHF)
Chronic obstructive pulmonary disease (COPD)
Right coronary artery (RCA) disease
Peripheral vascular disease
Left ventricular hypertrophy (LVH)
Left atrial enlargement
Electrocardiographic features
Renal failure
Moderate or severe aortic atherosclerosis
Withdrawal of
β
-blocker or ACEI
Body surface area (BSA)
Obesity and metabolic syndrome
Intra-operative
Aortic cross-clamp time
Bicaval canulation
Pulmonary vein venting
Type of surgery
Need of perioperative IABP
CPB time
CPB inclusive of cardioplegic arrest
Systemic hypothermia
Post-operative
Respiratory compromise
Red cell transfusion
Atrial fibrillation
Optimise fluid balance
Correct anaemia/hyperglycaemia/hypoxia
Correct electrolyte abnormalities
Wean inotropes
Sedation/analgesia
Haemodynamically
stable and rate
controlled
Observe 24 hours for
spontaneous resolution
Rapid ventricular
response/
haemodynamically
unstable
DC cardioversion
Amiodarone infusion
Peri-operative
β
-blockers and statins
Fig. 3.
Proposed strategy for the immediate treatment of AF
post cardiac surgery.