


















 41 / 66
41 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 6, November/December 2014
AFRICA
291
In black hypertensive patients a diuretic and/or a CCB is
recommended.
23
Beta-blockers should generally be avoided in
combination with diuretics as first-line therapy because of
predisposition to diabetes,
9
but this may not apply to highly
selective beta-blockers. Beta-blockers may also be considered if
there is intolerance to one of the first-line drugs. Loop diuretics
such as furosemide should not be used because of their short
duration of hypotensive activity of about six hours, unless there
is evidence of chronic kidney disease (CKD) with estimated
glomerular filtration rate (GFR)
<
45 ml/min.
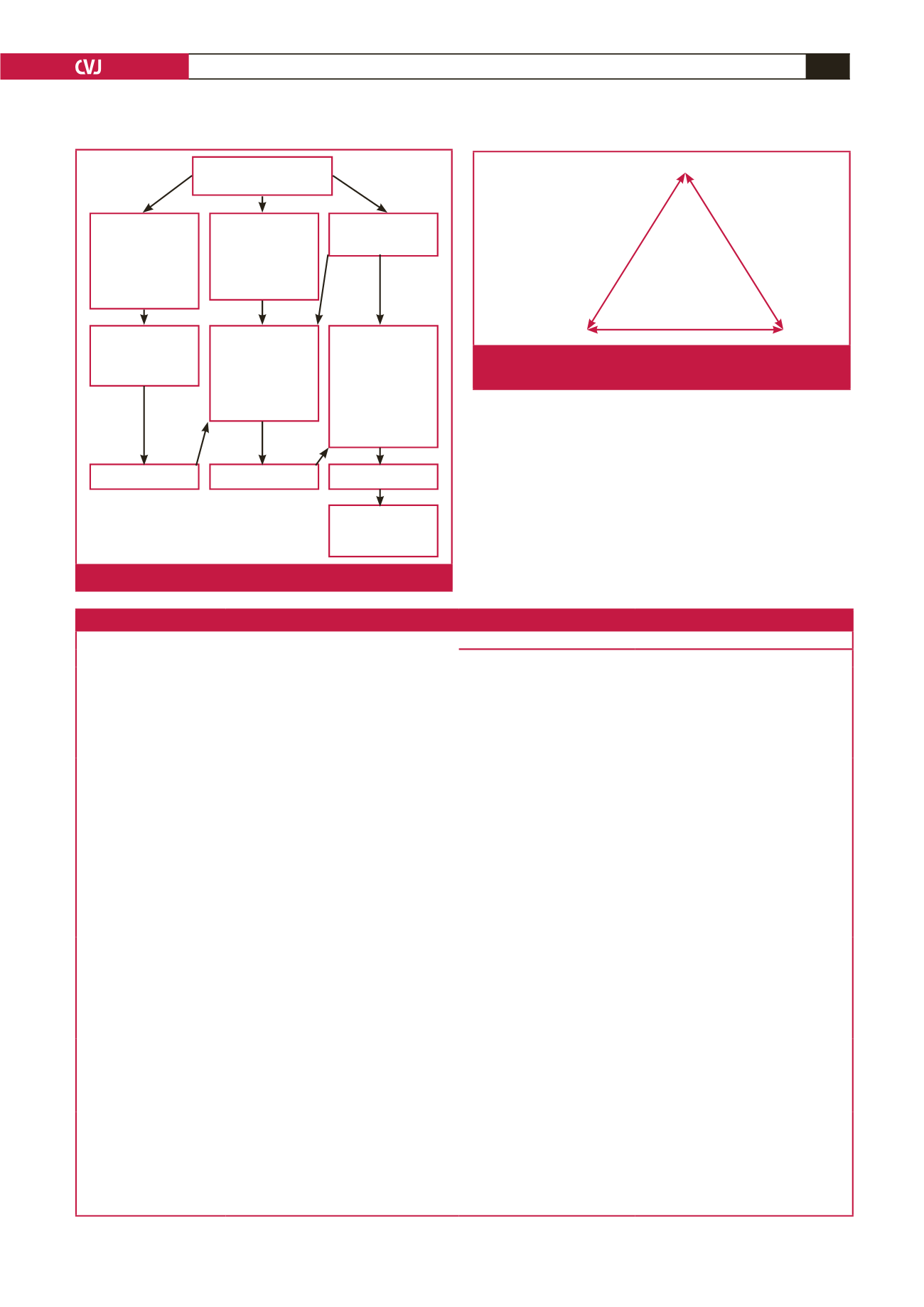
Measure BP on at
least three occasions
BP 140–159/
90–99 mmHg
with ≥ 3 risk
factor, diabetes,
TOD or
complications
BP ≥ 160/
100 mmHg*
BP 140–159/
90–99 mmHg
with < 3 risk
factors, no TOD
or complications
Lifestyle
modification and
commence two
drugs preferably
in fixed-drug
combination,
review in 4–6
weeks
Lifestyle
modification
and commence
monotherapy,
review in 4–6
weeks
Lifestyle
modification for
3–6 months
Not at goal
Not at goal
Not at goal
Add third drug/
optimise doses of
drugs
*BP > 180/110 mmHg refer to section 9
Fig. 1.
Overview of approach to treatment.
ACEI or ARB
Thiazide or
thiazide-like
CCB
Fig. 2.
Initial choices of antihypertensive treatment or combi-
nations.
Table 7. Indications and contra-indications for the major classes of antihypertensive drugs. Adapted from the ESC/ESH guidelines
9
Class
Conditions favouring the use
Contra-indications
Compelling
Possible
Diuretics (thiazide;
thiazide-like)
• Heart failure( HF)
• Elderly hypertensives
• Isolated systolic HTN (ISH)
• Hypertensives of African origin
• Gout
• Pregnancy
•
β
-blockers (especially atenolol)
Diuretics (loop)
• Renal insufficiency
• HF
• Pregnancy
Diuretics (anti-aldoste-
rone)
• HF
• Post-myocardial infarction
• Resistant hypertension
• Renal failure
• Hyperkalaemia
CCB (dihydropyridine)
• Elderly patients
• ISH
• Angina pectoris
• Peripheral vascular disease
• Carotid atherosclerosis
• Pregnancy
• Tachyarrhythmias
• HF especially with reduced ejection
fraction
CCB non-dihydropyridine
(verapamil, diltiazem)
• Angina pectoris
• Carotid atherosclerosis
• Supraventricular tachycardia
• AV block (grade 2 or 3)
• HF
• Constipation (verapamil)
ACEI
• HF
• LV dysfunction
• Post-myocardial infarction
• Non-diabetic nephropathy
• Type 1 diabetic nephropathy
• Prevention of diabetic microalbuminuria
• Proteinuria
• Pregnancy
• Hyperkalaemia
• Bilateral renal artery stenosis
• Angioneurotic oedema (more
common in blacks than in
Caucasians)
ARB
• Type 2 diabetic nephropathy
• Type 2 diabetic microalbuminuria
• Proteinuria
• LVH
• ACEI cough or intolerance
• Pregnancy
• Hyperkalaemia
• Bilateral renal artery stenosis
β
-blockers
• Angina pectoris
• Post-myocardial infarction
• HF (carvedilol, metoprololol, bisoprolol,
nebivolol only)
• Tachyarrhythmias
• Asthma
• Chronic obstructive pulmo-
nary disease
• AV block (grade 2 or 3)
• Pregnancy (atenolol)
• Peripheral vascular disease
• Bradycardia
• Glucose intolerance
• Metabolic syndrome
• Athletes and physically active patients
• Non-dihydropyridine CCBs
(verapamil, diltiazem)