


















 49 / 66
49 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 6, November/December 2014
AFRICA
299
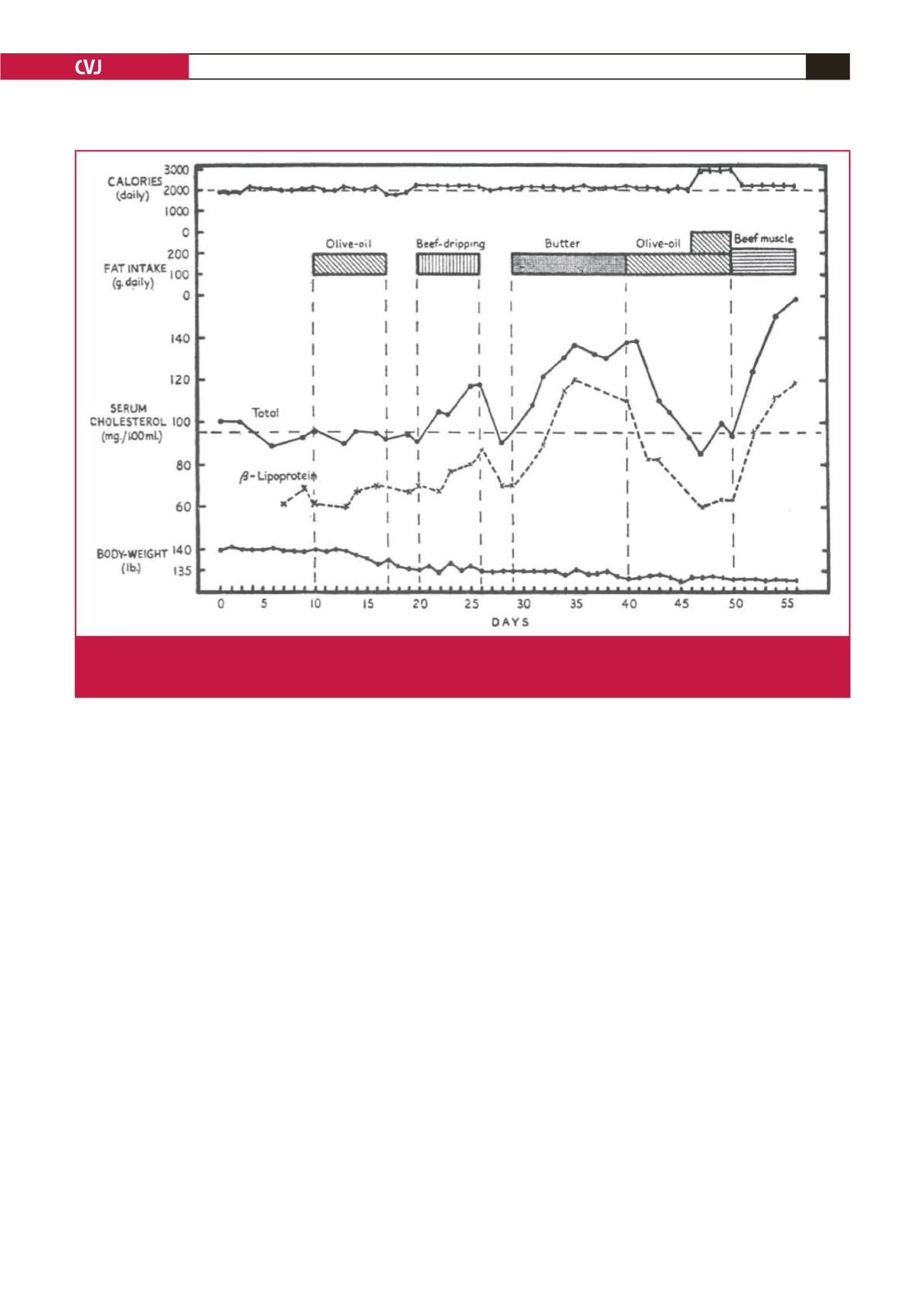
Town Department of Medicine used their specialised metabolic
unit to give a high-fat diet to subjects with an initially low blood
cholesterol level (Fig. 1).
12,13
A butter load of 100 grams given
daily increased blood cholesterol by proximately 40% within five
days. The addition of large amounts of olive oil to the butter
load restored cholesterol levels to their prior low levels (Fig. 1).
Therefore the type of fat diet affected blood cholesterol levels.
The decisive further link between circulating cholesterol
values and coronary heart disease came from the Framingham
study, which found that higher blood cholesterol values were
associated with increased cardiovascular and total mortality
rates.
15
Over time, the emphasis on selection of drug therapy via
statins has shifted to the blood level of low-density lipoprotein
(LDL) cholesterol.
16
In South Africa in 2000, high blood cholesterol levels have
been estimated to have caused 24 144 deaths (95% CI: 22 404–25
286) or 4.6% of all deaths.
17
Studies in the Cape Peninsula and
in the South African Indian population support links between
lipid abnormalities and coronary heart diseases.
18,19
Severely
obese South African white women have greatly reduced values
for serum high-density lipoprotein (HDL) cholesterol or ‘good’
cholesterol, rather than high levels of LDL cholesterol.
20
Lipids in diabetes: the role of statins
The ideal approach to nip diabetes in the bud is by testing HbA
1c
values in those with the metabolic syndrome or obesity, and then
to go for weight loss induced by combined diet and exercise.
In those with established type 2 diabetes (DM2), a population
study in Hong Kong suggested that statin therapy attenuated
the associated increased cancer risk.
21
For diabetes, in a large
study with 215 725 person-years of follow up, statin use before
the diagnosis of diabetes reduced diabetic retinopathy (hazard
ratio 0.60, 95% CI: 0.54–0.66;
p
< 0.0001), diabetic neuropathy
(HR 0.66, 95% CI: 0.57–0.75;
p
< 0.0001), and gangrene of the
foot (HR 0.88, 95% CI: 0.80–0.97;
p
= 0.010).
22
Regarding the
general adult population, statins are recommended as first-line
therapy in those up to and including 75 years of age, who have
clinical atherosclerotic cardiovascular disease (ASCVD) (Table 4
in Stone
et al
.
23
).
Exercise versus drugs
In studies on the secondary prevention of coronary heart
disease and pre-diabetes, randomised trials on exercise
interventions suggest that exercise and many drug interventions
are often potentially similar in terms of their mortality benefits,
rehabilitation after stroke, treatment of heart failure, and
prevention of diabetes.
24
This important observation reinforces
the essential role of exercise in any programme aimed at overall
cardiovascular health (Table 1).
Banting first linked diet to mortality
Banting in his pamphlet
25
in 1869 emphasised the role of diet
in weight loss, stating that: ‘The dietary is the principle point in
Fig 1.
A historical study in Cape Town. The effect of dietary fats on blood lipid levels and their relation to ischaemic heart disease,
neutralised by the effect of added olive oil. Note the rapid rise in serum cholesterol levels with the provision of the high-butter
diet. All values were obtained in the Metabolic Unit, University of Cape Town, South Africa. From Bronte-Stewart.
14