


















 28 / 68
28 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 1, January/February 2015
26
AFRICA
and stent. PTCA only was performed in four of the patients.
Complete revascularisation is the first priority universally for
all patients in cardiac surgery, so these were all candidates for
redo CABG. The reason for ischaemic symptoms in six of our
patients was graft occlusion, new lesions in 19, and both in seven
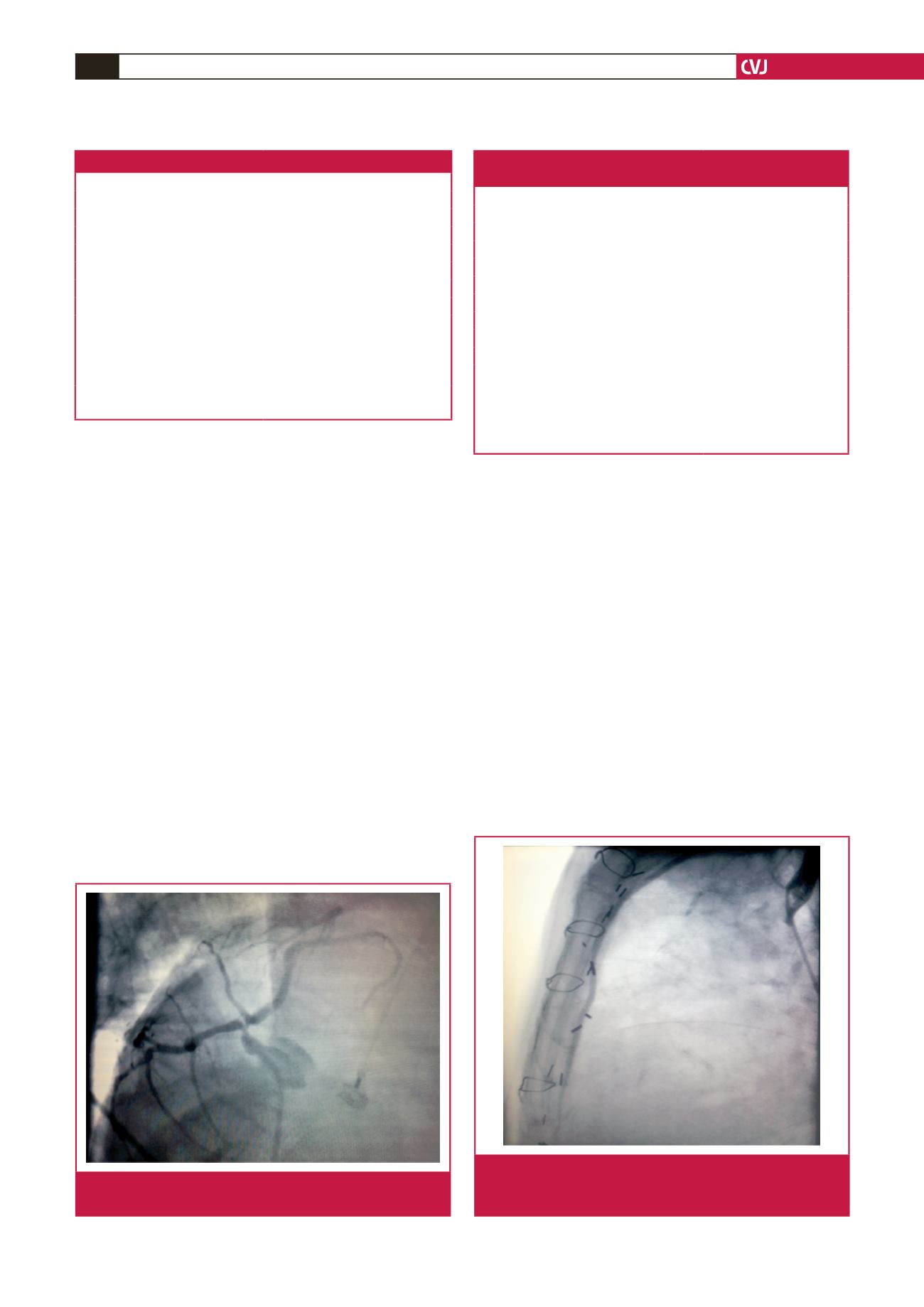
(Table 2). New lesions occurred in the left main coronary arteries
of eight patients (Fig. 1), and in the rest, in branches of the Cx.
We decided to perform an off-pump posterolateral
thoracotomy for redo CABG in these patients because of
the presence of patent grafts (Fig. 2), to avoid the risks
of resternotomy, and to access the posterior region of the
heart more easily while revascularising the branches of the Cx
system. One of the most significant independent predictors of
morbidity and mortality after redo CABG is reported to be
long duration of CPB.
6
We therefore decided to avoid CPB and
chose the off-pump redo CABG technique via a thoracotomy for
revascularising the lateral aspect of the heart.
All patients underwent redo off-pump CABG via a left
posterolateral thoracotomy (Fig. 3) with general anaesthesia
after insertion of a double-lumen endotracheal tube. The patient
was positioned in the right lateral decubitus position with the
pelvis externally rotated slightly to allow access to the femoral
vessels for cannulating the patient if necessary. The saphenous
veins (SV) or radial arteries (RA) were prepared as grafts at the
same time as the thoracotomy, from the contralateral extremity,
without any positional problems. A supine position before
thoracotomy was necessary in only one patient for harvesting
the SV because the right SV had been harvested before. In six
patients, the SV was harvested and in the rest the RA was used.
A left posterolateral thoracotomy was performed through
the fifth intercostal space and adhesions of the collapsed left
lung were dissected. After mobilisation of the left lung, the
pericardium was opened above the target area, taking care with
the phrenic nerve and LITA graft, which was patent in all our
patients. We limited dissection of the adhesive tissues because
extensive dissection may cause increased venous bleeding and a
decrease in the natural stabilisation provided by the adhesions in
redo CABG patients.
7
After graft preparation, the proximal anastomosis was
performed by placing a side-biting clamp on the descending aorta
Table 1. Pre-operative demographic data
Variables
Demographic data (
n
= 32)
Age (years) (mean)
61.66
±
8.63 (40–76)
Male,
n
(%)
27 (84.4)
Female,
n
(%)
5 (15.6)
Hypertension,
n
(%)
21 (65.6)
Smoking,
n
(%)
21 (65.6)
Diabetes mellitus,
n
(%)
13 (40.6)
Family history,
n
(%)
22 (68.7)
Hyperlipidaemia,
n
(%)
22 (68.7)
Myocardial infarction,
n
(%)
11 (34.3)
COPD,
n
(%)
6 (18.7)
CVA,
n
(%)
2 (6.2)
COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular
accident.
Table 2. Information on the patients after the first operation up
to the redo Cx CABG via thoracotomy
Variable
Number
±
SD
Number of previous grafts
2.1667
±
1.019
Patent anastomoses
LIMA–LAD
32
RCA
10
Cx
2
Reason of redo Cx CABG
Graft occlusion
6
New lesion
19
Both
7
Interventions
PTCA
4
PTCA + stent
6
Period between the first and redo CABG
via thoracotomy operation (months)
103.03
±
63.33
Fig. 1.
New lesion in the left main coronary artery of a patient
with a patent LITA–LAD anastomosis.
Fig. 2.
Extremely adhesive LITA lying under the sternum,
a good example of an indication for redo CABG via
posterolateral thoracotomy.