


















 65 / 68
65 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 1, January/February 2015
AFRICA
e15
and calcium gluconate for prevention of pre-eclampsia, and
therapeutic enoxaparin for the thrombus in the descending aorta.
First-trimester foetal aneuploidy screening was negative and
the foetus was also structurally normal. The patient was seen
every two weeks at the cardiac-obstetric unit for evaluation of
blood pressure, urinalysis and foetal growth. An echocardiogram
was done monthly to evaluate the aorta for disease progression.
The antenatal course was uneventful. The blood pressure was
well controlled (around 130/70 mmHg) with appropriate foetal
growth. The patient was delivered by elective caesarean section
with spinal anaesthesia at 34 weeks’ gestation. A healthy baby
weighing 2.3 kg with good Apgars was delivered. The mother
was observed in a high-dependency unit for 24 hours after
delivery where her blood pressure remained well controlled.
After delivery, treatment with prednisone, azathioprine and
enoxaparin was continued, methyl-dopa was stopped and
nifedipine re-started and stool-softeners were also prescribed.
The patient was discharged five days after delivery. Repeat CT
angiography and echocardiogram at the six-week postnatal visit
was unchanged.
Discussion
Takayasu arteritis was first described in 1908 by the Japanese
ophthalmologist who observed retinopathy in the absence of
peripheral pulses. Autoimmunity, sex hormones (more common
in females) and a genetic predisposition of the human leucocyte
antigen have been proposed as possible causes.
5
The disease is classified clinically into stages depending on
the presence of complications such as hypertension, retinopathy,
aneurysms and aortic insufficiency: group I, uncomplicated
disease; group IIa, single complication with uncomplicated
disease; group IIb, severe single complication with uncomplicated
disease; group III, two or more complications with uncomplicated
disease.
6
Our patient had group III disease.
Patients with Takayasu disease should be managed in a high-
risk obstetric unit. Pregnancy is not associated with disease
progression, however there is a 60% risk of complications
developing during pregnancy.
7
Maternal risks are attributed
mainly to arterial hypertension, and the most important risks
include development of pre-eclampsia, exacerbation of chronic
hypertension, heart failure, and cerebral vascular accidents.
8
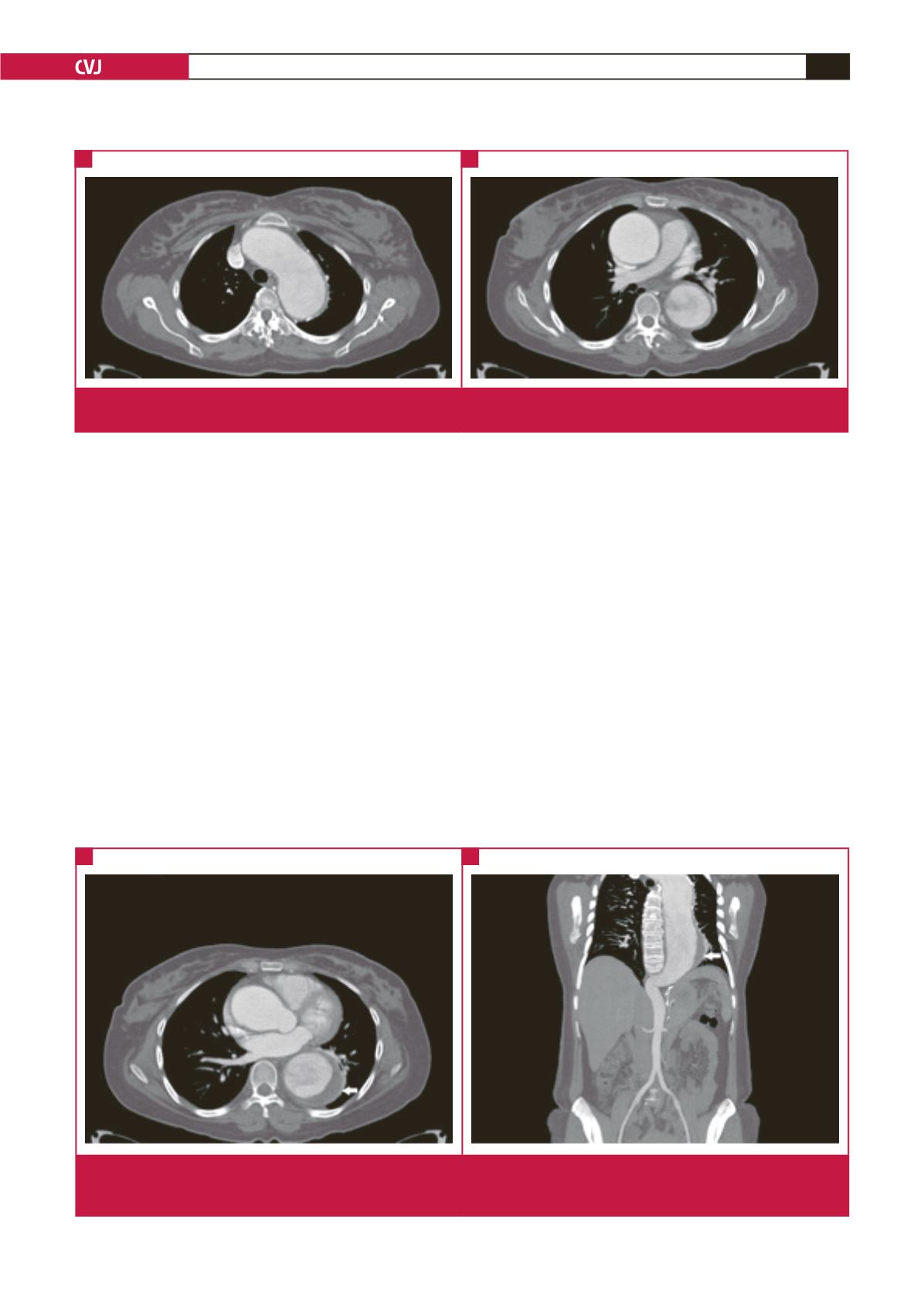
Fig. 1.
Axial CT post-contrast images in the arterial phase demonstrating aneursymal dilatation of the arch of the aorta (A) and the
ascending and descending aorta (B). Note the turbulent flow in the descending aorta.
A
B
Fig. 2.
Post-contrast CT images (A) in the axial post-contrast venous phase and (B) coronal curved reconstruction in the arterial
phase demonstrating marked thickening of the wall of the thoracic aorta (arrows). Note the involvement of the thoracic aorta
only, with sparing of the abdominal aorta.
A
B