
















 19 / 68
19 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 3, May/June 2015
AFRICA
117
compared to healthy controls, but there was no significant
difference between the MP users and cigarette smokers. Also,
the amount of MP used and cigarette smoking (pack years) was
correlated with LAAEV and LAAEF. This is the first study to
determine the atrial electromechanical and mechanical functions
of MP users and cigarette smokers.
Cigarettes have widespread use and their smoke contains
more than 4 000 toxic compounds, mainly nicotine. Various
clinical and pathological investigations have shown that cigarette
smoking caused atherosclerosis, myocardial infarction and heart
failure,
4
and nicotine abuse is associated with the occurrence of
cardiac arrhythmias.
9,12
The pro-arrhythmic effect of cigarette
smoking seems to depend on the nicotine concentration in the
blood.
9
Increased nicotine levels increase atrial and ventricular
vulnerability to fibrillation.
9,12
These effects are more likely
to depend on the inhibition of ion channels and conduction-
slowing properties.
One factor known to cause a substantial slowing of electrical
impulse propagation in cardiac tissue is an increase in the
amount of interstitial collagen. It has been found that the
prolonged administration of nicotine is also associated with the
loss of intracellular K
+
and the emergence of cardiac necrosis.
21
Experimentally, Goette
et al
. established a linear correlation
between nicotine dose and atrial collagen expression, leading
to symptomatic atrial fibrosis at a younger age.
22
In previous
reports, atrial conduction time was found to be prolonged
independently of LA dilatation.
20,23
In a study consisting of
50 smokers and 40 non-smokers, it was found that inter- and
intra-atrial electromechanical delay was significantly higher
in cigarette smokers compared with non-smokers, and the
amount of smoking was strongly correlated with inter-atrial
electromechanical delay.
24
Distinct from that study, our study contained a third group, the
MP users, and we also investigated left atrial mechanical function
in our study population. Likewise, we found that although LA
was not dilated, atrial conduction time was prolonged in both
MP users and smokers. This may be explained as the negative
effects of nicotine on cardiac structure and function. The
development of interstitial fibrosis affects chamber geometry
and mechanical performance of the heart and enhances the
likelihood of cardiac arrhythmias, such as atrial fibrillation
(AF). Moreover, in prospective, population-based and 16-year
follow-up studies, it has been shown that smoking was associated
with incidence of AF, with more than a two-fold increased risk
of AF attributed to current smoking.
25
The risk of AF increased
with increasing cigarette years of smoking, and appeared to be
somewhat greater among current smokers than former smokers
with similar cigarette years of smoking.
25
MP is a form of smokeless tobacco. The ash in this mixture
transforms the alkaloids into a base form and provides easy
absorption from the buccal mucosa.
26
As MP contains six- to10-
fold more nicotine than cigarettes, it is preferred by addicts. It
has been shown that urinary cotinine levels were three times
higher in MP users than in cigarette smokers.
27
Besides, MP is
closely associated with traditional cardiovascular risk factors
and endothelial dysfunction, as detected by low plasma NO
levels.
3
MP increases oxidative stress and lipid peroxidation
levels, which are the best indicators of cytological damage.
28
Because of the deleterious effects of cigarette smoking,
especially the nicotine blood level, it stimulates the sympathetic
nerve endings and increases adrenaline release, which in turn
increases cardiovascular abnormalities.
29
The probability
of abnormalities of the cardiac conduction system and the
Table 3. Findings of atrial electromechanical coupling
measured by tissue Doppler imaging
Group I
controls
(
n
=
50)
Group II
smokers
(
n
=
50)
Group III
MP users
(
n
=
50)
p
-value
Lateral PA (ms)
48.3
±
9.8 53.9
±
12.9 54.1
±
14.1
§
0.032
Septal PA (ms)
40.1
±
8.7 46.3
±
13.3
#
45.8
±
15.2 0.028
RV PA (ms)
34.1
±
8.4 38.4
±
9.9 37.5
±
12.7 0.098
Lateral PA–septal PA (ms)
8.1
±
3.5
7.9
±
4.3
8.2
±
3.9 0.687
Lateral PA–RV PA (ms)* 14.2
±
8.9 15.5
±
10.1 16.5
±
8.4 0.443
Septal PA–RV PA (ms)** 6.0
±
5.9
7.9
±
8.8
8.2
±
7.7 0.287
PA: the interval with tissue Doppler imaging, from the onset of P wave on the
surface electrocardiogram to the beginning of the late diastolic wave (Am wave).
*Inter-atrial dyssynchrony, **intra-atrial dyssynchrony.
§
p
=
0.05 versus group I,
#
p
=
0.04 versus group I.
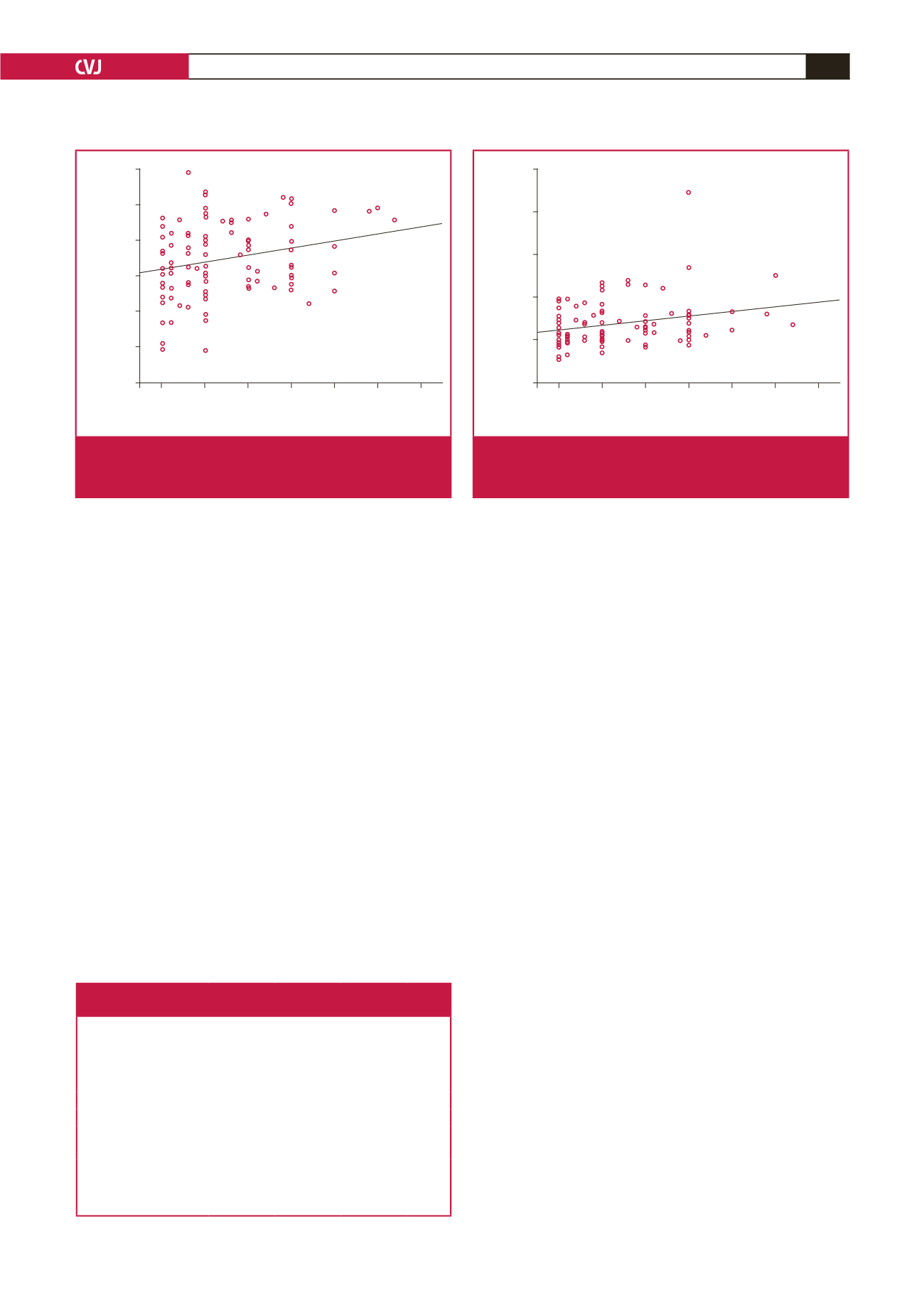
0.70
0.60
0.50
0.40
0.30
0.20
0.10
5.00 10.00 15.00 20.00 25.00 30.00 35.00
Duration (pack years)
Left atrial active emptying fraction (%)
R
2
linear
=
0.061
Fig. 1.
This shows positive correlations between LA active
emptying fraction and the amount of MP use and cigarette
smoking (pack years) (
r
=
0.25,
p
=
0.013).
25
20
15
10
5
0
5.00 10.00 15.00 20.00 25.00 30.00 35.00
Duration (pack years)
Left atrial active emptying volume (cm
3
/m
2
)
R
2
linear
=
0.069
Fig. 2.
This shows positive correlations between LA active
emptying volume and the amount of MP use and cigarette
smoking (pack years) (
r
=
0.26,
p
=
0.009).