
















 46 / 68
46 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 3, May/June 2015
144
AFRICA
at the time of pacemaker implantation, including antibiotics and
anaesthetics. Ginwalla
et al
.,
3
for example, described a case of
haloperidol-induced TdP in a patient with complete AV block.
The haloperidol was given to control agitation in an elderly
gentleman, which resulted in TdP requiring defibrillation and
intravenous magnesium.
Their case and ours highlights the importance of doctors
needing to be aware of what medications and electrolyte
imbalances to avoid in patients with severe bradyarrhythmias.
Our case highlights the care required in the peri-operative
patient with complete AV block who may receive a number of
potentially hazardous drugs.
It has been known for many years that erythromycin
prolongs the QT interval in susceptible individuals and can
lead to potentially fatal dysrhythmias.
5
The mechanism of QT
prolongation due to erythromycin is related to blockade of
potassium efflux in the plateau phase of the myocardial action
potential.
6.7
Daleau
et al.
8
were the first to demonstrate that the
effect of erythromycin is to inhibit the rapid component of the
delayed rectifier current (I
Kr
) in guinea pig myocytes.
Prolongation of the action potential increases the risk of
early after-depolarisations in M cells deep within the ventricular
myocardium and creates marked dispersion of repolarisation
across the ventricular wall.
7
This sets the stage for maintaining
the characteristic spiraling ventricular arrhythmia, TdP. The
development of right ventricular ectopic beats during temporary
pacemaker insertion can create the classic ‘short–long’ R–R
intervals associated with polymorphic ventricular tachycardia
initiation, which is then maintained by the erythromycin-induced
dispersion of repolarisation.
The mechanism of QT prolongation in patients with
bradycardia-related TdP is poorly understood. Certainly, not
all patients with AV block get prolongation of the QT or TdP.
Kurita
et al
.
9
demonstrated that patients with complete AV
block with TdP have a bradycardia-sensitive repolarisation
abnormality, which persists even after pacemaker implantation.
However, there is little data on the actual mechanism responsible
for QT prolongation and it may just be that those individuals
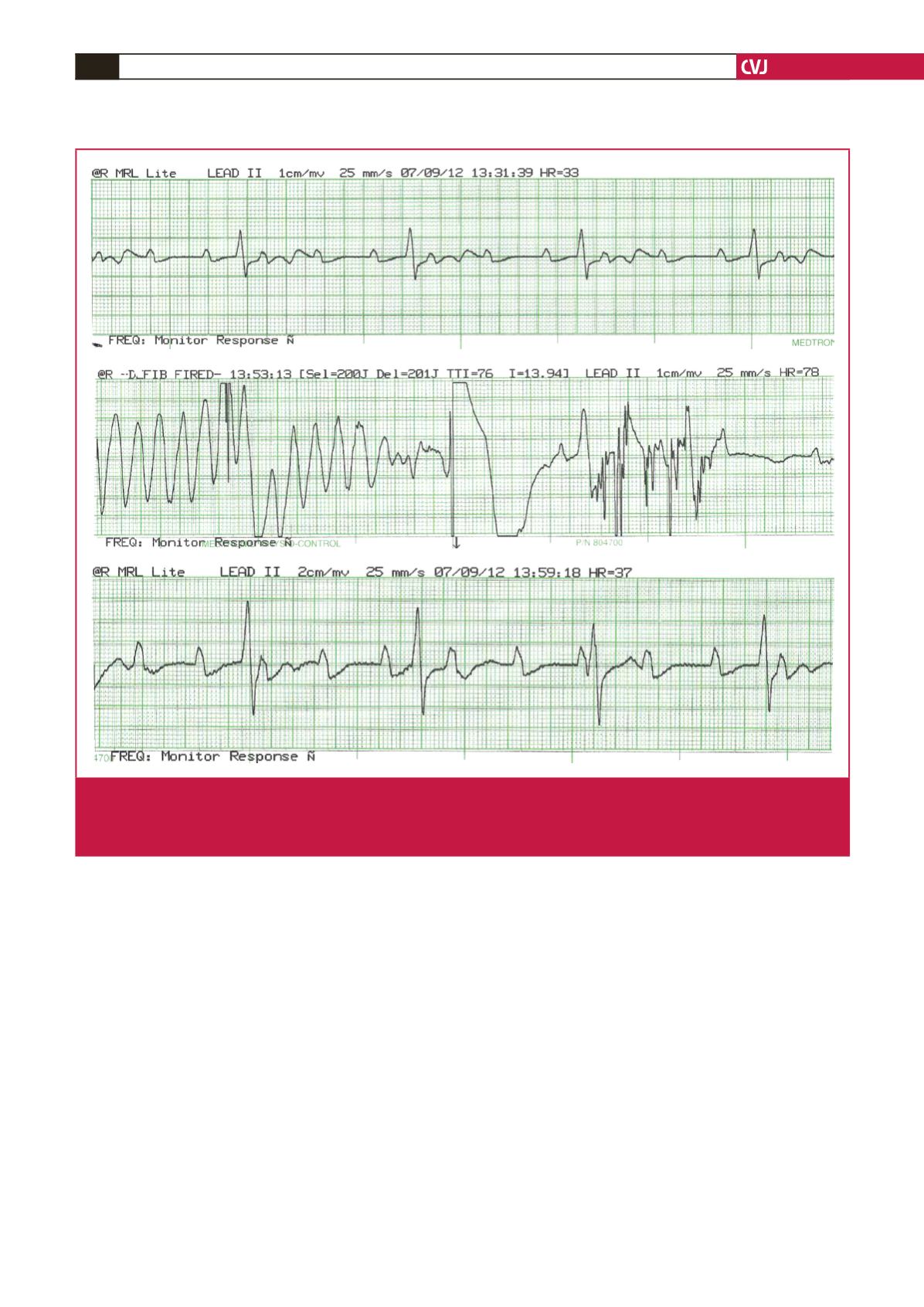
Fig. 1.
This shows the rhythm strip of the patient prior to administration of erythromycin (top strip), during direct-current cardiover-
sion for torsade de pointes (middle strip), and after successful cardioversion (bottom strip). At baseline (top strip) the ECG demon-
strates complete heart block with an uncorrected QT interval of 600 ms. The middle strip clearly demonstrates TdP, which is treated
with electrical cardioversion in the centre of the middle strip, followed by return to the baseline dysrhythmia in the bottom strip.