
















 34 / 64
34 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 1, January/February 2016
32
AFRICA
Complete vascular rings may be divided into four major
configurations, with double aortic arch being the most frequent
variation encountered, followed by right aortic arch with
aberrant left subclavian artery and left ligamentum.
2
Innominate
artery compression and pulmonary vascular slings are other
configurations infrequently seen.
2,3
Double aortic arches may
present with earlier clinical symptoms than other configurations.
2
In a symptomatic patient with a vascular ring, the plain
chest radiograph will invariably demonstrate some abnormality.
1
On the frontal film, the presence of a right aortic arch, right
descending aorta or focal tracheal indentation should be noted,
while the lateral chest radiograph may illustrate anterior tracheal
bowing, increased retrotracheal soft tissue opacification, as well
as focal tracheal narrowing.
1,4
A high kV magnification technique
may be used to exclude tracheal narrowing on the plain chest
radiograph.
4
The aortic arch may not be clearly visualised on
frontal CXR in infants due to obscuration by the thymic shadow.
3
Although useful to prompt further imaging, these signs
are not useful to identify the specific type of vascular ring
configuration. The frontal CXR mediastinal silhouette of any
child with aerodigestive tract symptoms should always be
carefully scrutinised despite an apparently obvious alternative
aetiology, such as a foreign body.
6
The contrast oesophagogram is useful to exclude the presence
of a vascular ring, particularly in patients with persistent asthma
or aspiration symptoms unresponsive to standard treatment.
3
A
persistent, extrinsic pulsatile indentation seen in multiple views
during a contrast study of the oesophagus (generally laterally
with double aortic arches and anteriorly with pulmonary artery
sling) is highly suggestive of a vascular ring, while a normal
study effectively excludes the diagnosis of a vascular ring.
4
Occasionally an alternative diagnosis, such as aspiration or
tracheo-oesophageal fistula, may be identified.
3
CO is widely available, cheap and relatively non-invasive,
all important characteristics in underdeveloped areas of South
Africa, where access to advanced imaging may require referral to
a tertiary centre a significant distance away.
While CXR and CO may confirm the presence of a vascular
ring, cross-sectional imaging is required to confirm the specific
configuration of the ring and enable surgical planning, and
to exclude another cause of a fixed extrinsic oesophageal
indentation, such as a mediastinal foregut duplication cyst.
5,6
Detailed cross-sectional imaging, in the form of computed
tomography angiography or magnetic resonance imaging, is
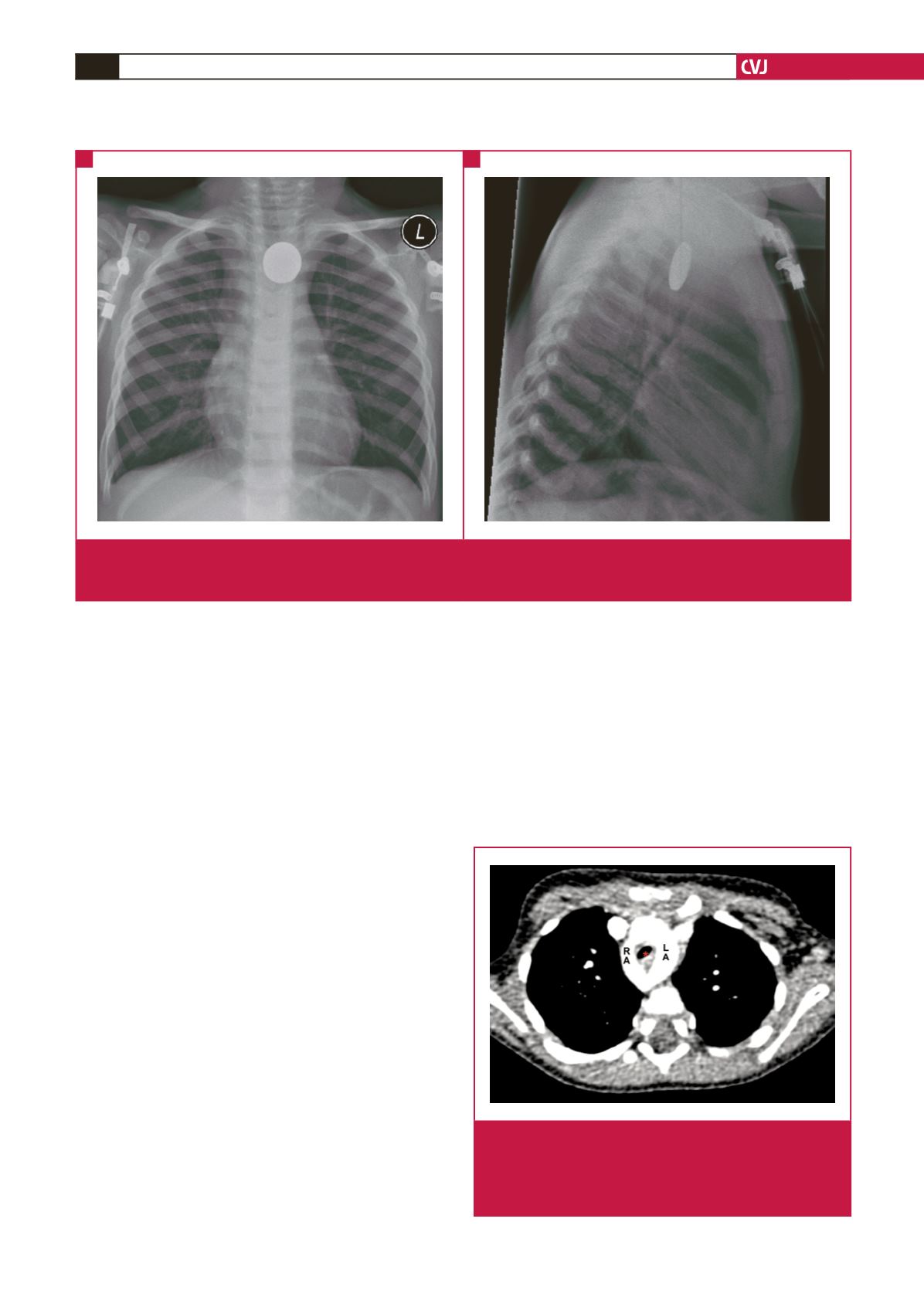
Fig. 1.
Red herrings. (A) The postero-anterior and (B) lateral plain chest radiographs illustrate the ingested coin in the oesophagus,
superimposed on a widened superior mediastinal silhouette. The stridor persisted following extraction of the coin, prompting
a computed tomography angiogram (CTA) that confirmed a double aortic arch.
A
B
Fig. 2.
Double aortic arch. This axial CTA image illustrates the
characteristic appearance of a double aortic arch, with
both arches widely patent and contrast enhanced. The LA
and RA encircle the oesophagus and trachea (asterisk) to
form a complete vascular ring. LA: left arch; RA: right arch.