
















 35 / 64
35 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 1, January/February 2016
AFRICA
33
a crucial aspect of illustrating the detailed ring configuration
and to facilitate surgical planning.
3
Patent vascular channels
are evident on CTA as contrast-enhancing segments, and are
well visualised on reconstructed images (Figs 2, 3). Conversely,
atretic vascular segments and ligaments are not evident on
contrast-enhanced images (Figs 4, 5), but their presence can
be inferred from traction on associated vascular structures or
compression of the trachea.
4
The ‘four-artery sign’ is a useful
CTA radiographic sign which indicates an abnormal aortic
branching pattern and is suggestive of a vascular ring.
4
CTA allows multi-planar views to be obtained, with three-
dimensional reconstructions clearly illustrating vascular and
tracheal relationships. CTA also allows detailed evaluation
of the lung fields, particularly in patients with co-existing
pulmonary disease.
7
Inspiratory and expiratory CTA studies
allow the dynamic evaluation of tracheal calibre for narrowing
or traction, which is particularly important in patients with
associated tracheo- or bronchomalacia.
2,3,8
CTA is generally easily accessible and diagnostic interpretation
relatively straightforward.
2
CT scanning times are shorter than
MRI and therefore sedation is usually not necessary, a significant
advantage in a stridulous patient.
2,4
The principle disadvantages
of CTA are the need for intravenous contrast agents, and the
potential late consequences of radiation-dose exposure.
9
Vascular ring patients are only exposed to a single CTA, as
serial imaging is not indicated before or after surgery. In the
absence of basic investigations (CXR and CO) consistent with
a vascular ring, CTA should not be used as a screening tool to
exclude the diagnosis, except in a critically ill patient in whom the
diagnosis is considered.
Like CTA, MRI is a sensitive imaging tool for visualising
vascular ring configuration. Advantages of MRI over CTA
include the freedom from exposure to both radiation and
intravenous contrast, as well as the ability to undertake
haemodynamic studies in patients with intracardiac lesions.
The limitations of MRI include the longer scanning time
than CTA, the need for sedation in paediatric patients, and
limited accessibility and reporting expertise in the developing
world. Sedating patients with stridor resulting from a vascular
ring requires rigorous monitoring to avoid potential airway
obstruction, and is usually undertaken by specially trained
nursing staff and in some instances senior MRI specialists.
10
Endotracheal intubation is avoided to allow accurate tracheal
cross-sectional evaluation.
2
MRI demands more in terms of
human resources, expertise and time. Despite its availability at
our institution, CTA remains the favoured modality to obtain
cross-sectional imaging of both the vascular ring and the
trachea.
Echocardiography is used principally to investigate
intracardiac abnormalities that will be present in approximately
12.4% of vascular ring patients.
2
However, echocardiography is
a poor imaging tool to either establish or exclude the diagnosis
of a vascular ring due to poor acoustic windows, ligamentous
structures and hyperinflation of the lungs.
2,8
In the past, conventional catheter angiography (CCA) was
used, in conjunction with CXR and CO, to elucidate the exact
configuration of a vascular ring and thus plan surgery. In the
current era, non-invasive imaging modalities are preferred and
CCA is reserved for the investigation of concomitant intracardiac
lesions to obtain angiographic and haemodynamic data.
4
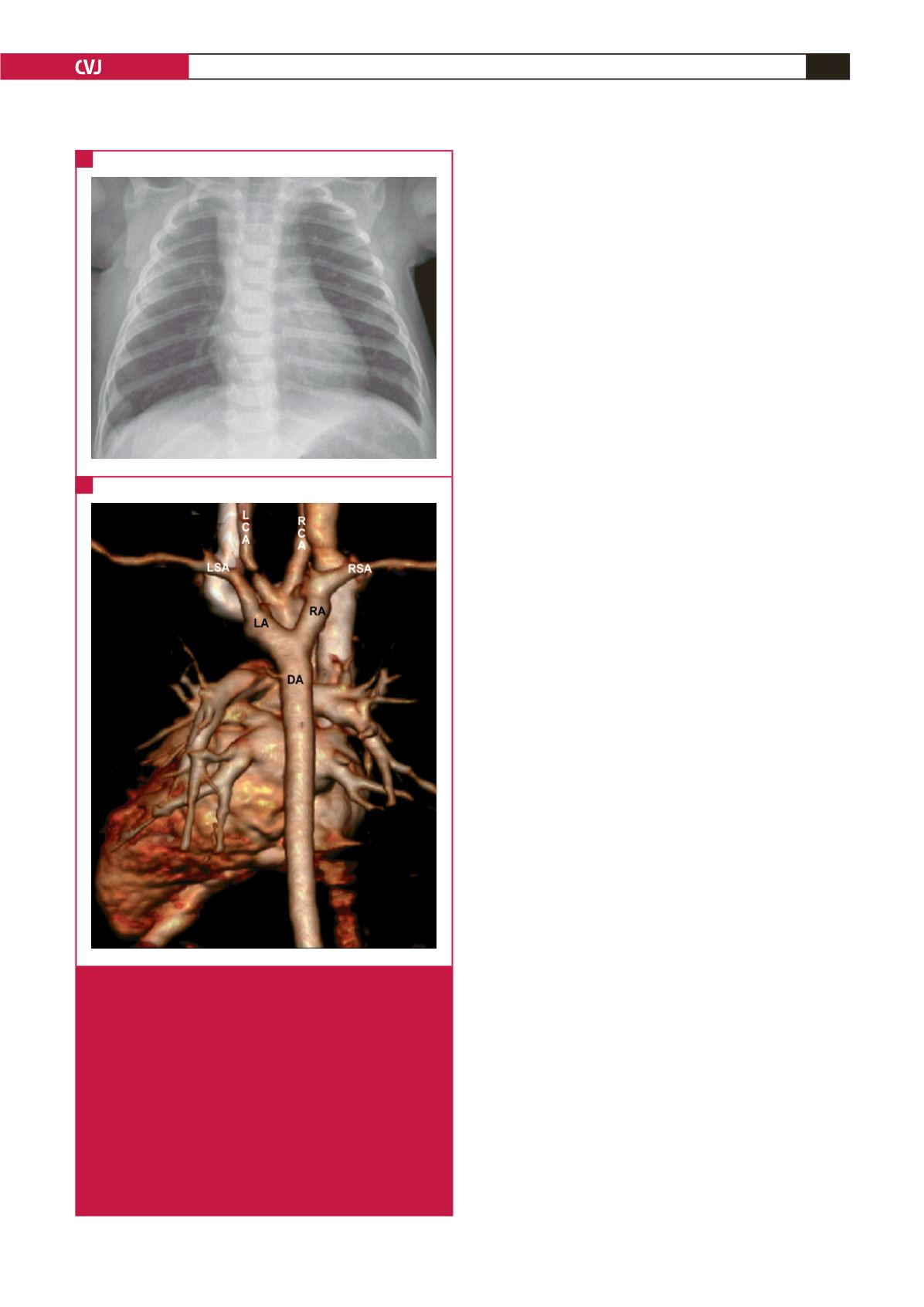
Fig. 3.
Double aortic arch with both arches patent. (A) The
plain chest radiograph demonstrates a widened supe-
rior mediastinal silhouette, with the presence of a right
aortic arch in this child with stridor and dysphagia.
(B) The reconstructed postero-anterior CTA image
illustrates the double aortic arch, with the LA and RA
patent and of similar calibre at the confluence with the
DA. Clearly illustrated are the head and neck vessels,
which arise individually from their respective aortic
arches, hence the ‘four-vessel sign’ used to aid diag-
nosing a vascular ring radiologically. LA: left arch; RA:
right arch; DA: descending aorta; LSA: left subclavian
artery; LCA: left carotid artery; RSA: right subclavian
artery; RCA: right carotid artery.
A
B