
















 41 / 76
41 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 4, July/August 2018
AFRICA
239
invention needed a third revascularisation to be carried out. A
total of 16 patients (eight males and eight females) needed more
than three surgical interventions.
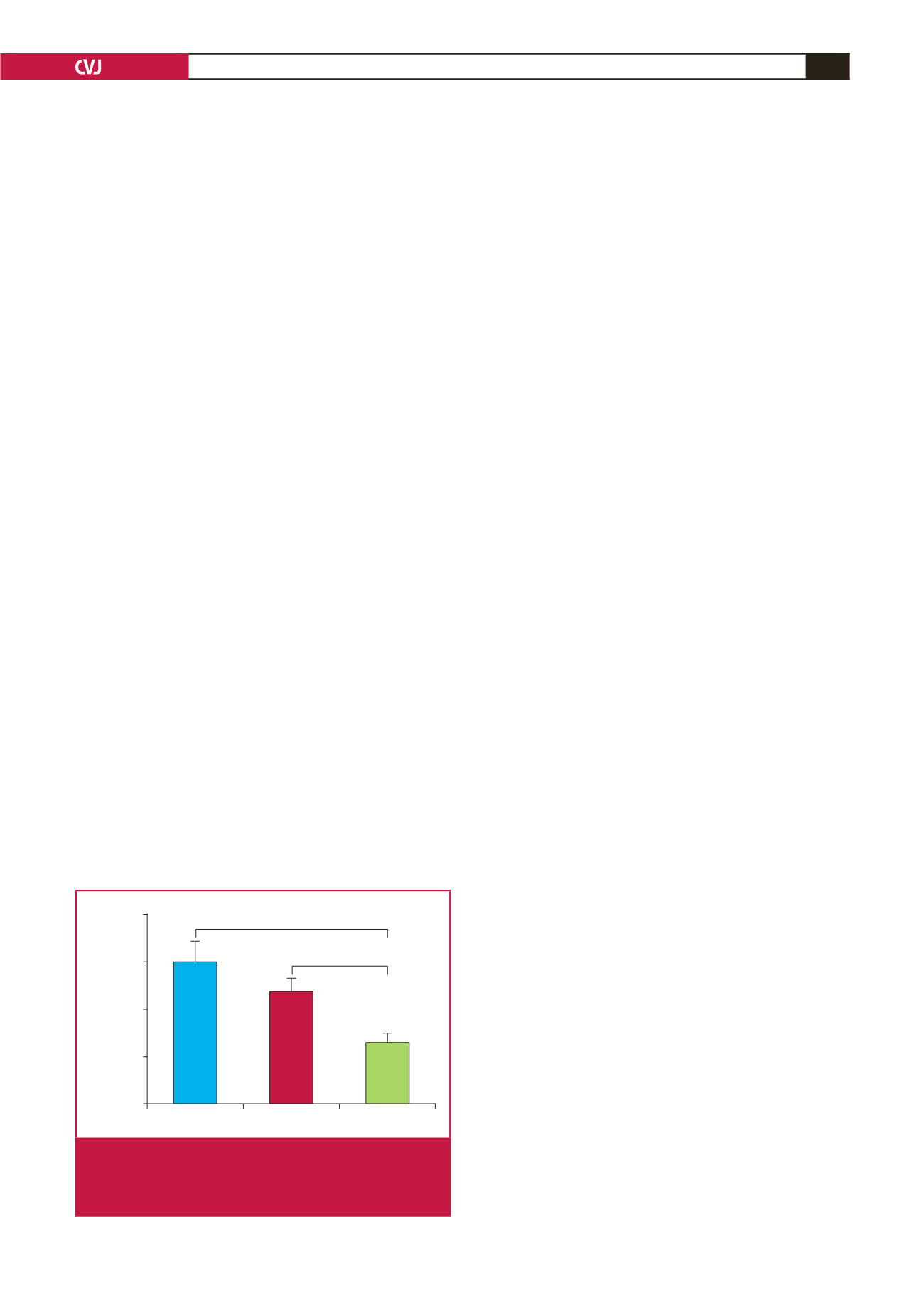
As depicted in Fig. 1, it took 60 months (five years) for
patients who were treated with OMT before their first surgical
intervention to require the second revascularisation. Those who
received SOMT and those who did not receive medication at all
before their first surgery took 48 and 26 months, respectively,
to require the second revascularisation. The differences (i.e.
34 months) between those who were on OMT and those who
did not receive any medical therapy before their first surgical
intervention were statistically significant (
p
<
0.001).
Similarly, the differences (22 months) between those who
were on SOMT and those who did not receive any medical
therapy before their first surgical intervention were statistically
significant (
p
<
0.05). The specific type of the first surgical
intervention had a significant (
p
<
0.05) impact on how long it
took for the second revascularisation to be needed. For example,
it took 138 months (about 11.5 years), 46 months (nearly four
years) and 18 months for patients who received CABG, BMS
and DES, respectively, to require the second revascularisation.
Discussion
The main findings of this study indicate that OMT is pivotal
in the management of stable angina pectoris. This is in support
of several recent studies that have shown that there were no
differences between PCIs and OMT with regard to the all
major outcomes in patients with stable angina pectoris.
21
What
is more exciting and novel about our findings, in addition to
corroborating other recent findings such as those reported by
Iqbal
et al.
, is that OMT reduces the need for subsequent PCIs
when used before or together with an appropriate surgical
intervention(s).
22
More importantly, this study has shown that
OMT lengthens the period between surgical interventions.
However, the average age (65 years) of patients in this study
might have played a role in these findings. Recently, Won and
colleagues reported that PCIs were more beneficial than OMT
in patients with stable angina pectoris, aged 75 to 85 years old.
23
It was regrettable, as shown by the findings of our study,
that 75% of patient aged 65 years old (on average), who might
have benefited immensely, were not treated with OMT as the
initial management approach. Furthermore, the use of OMT
in this study was significantly less than the 44% reported in
the COURAGE study.
19
However it was much better than the
17% reported from the New York State Registry.
21
Therefore,
it means that the vast majority of medical practitioners in
private healthcare settings in South Africa still prefer surgical
interventions as the initial management approach for stable
angina pectoris, although there is strong evidence to the contrary.
The barriers to effective implementation of clinical guidelines
and their uptake into routine clinical practice are well documented
worldwide.
24,25
For example, Grol and Grimshaw reported that
absence of facilities, lack of feasibility, old routines, heavy
work-load, as well as no immediate risk of consequences for
non-compliance were the main barriers for poor implementation
of evidence.
26
The latter offers a possible explanation for the lack of
implementation of the findings of the COURAGE trial
19
in
private healthcare settings in South Africa, as reported in
this study. In these settings, there are generally no immediate
consequences for medical practitioners not adhering to
clinical guidelines. This happens because other than the strict
requirements set by medical aid schemes in South Africa, mostly
each medical practitioner relies on his/her own expert judgement.
More importantly, ‘professional pride and payer profit’ have a
big impact on ‘perspectives on optimal care and the best method
for improving health care’.
27
Therefore, it is also possible that OMT was less favoured
in private healthcare settings because of its minimal financial
benefits for medical practitioners, compared to surgery. As a
result, the majority of cardiologists in private healthcare settings,
as was recently reported by Mohee and Wheatcroft, continue to
underestimate the benefits of OMT in patients with stable angina
pectoris.
28
There are some limitations to this study. As it often the case
with other retrospective studies, there were missing data from
the files of patients studied. Most notably, we could not assess
the impact OMT on survival because of missing mortality data.
However, there is a low prevalence of mortality due to stable
angina pectoris.
29,30
Therefore it is unlikely that lack of data on
survival rates in the population studied had a significant impact
on the findings of this study.
Conclusion
Compelling evidence suggests that OMT should be the initial
management approach in patients with stable angina. Therefore
a reasonable approach is to optimise OMT and reserve coronary
revascularisation for mainly older patients who are sub-optimally
controlled on medical therapy, or for patients who are at high
risk of major adverse cardiac events.
References
1.
Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, Murphy A.
Growing epidemic of coronary heart disease in low- and middle-income
countries.
Curr Problems Cardiol
2010;
35
(2): 72–115.
2.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman
M,
et al.
; American Heart Association Statistics Committee; Stroke
OMT
SOMT
No medication
Period (in months)
80
60
40
20
0
*
p
<
0.05
*
*
Fig. 1.
Period (in months) it took for groups of patients with
stable angina to require second surgical intervention.
OMT: optimal medical therapy; SOMT: sub-optimal
medical therapy.