


















 19 / 64
19 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 30, No 4, July/August 2019
AFRICA
205
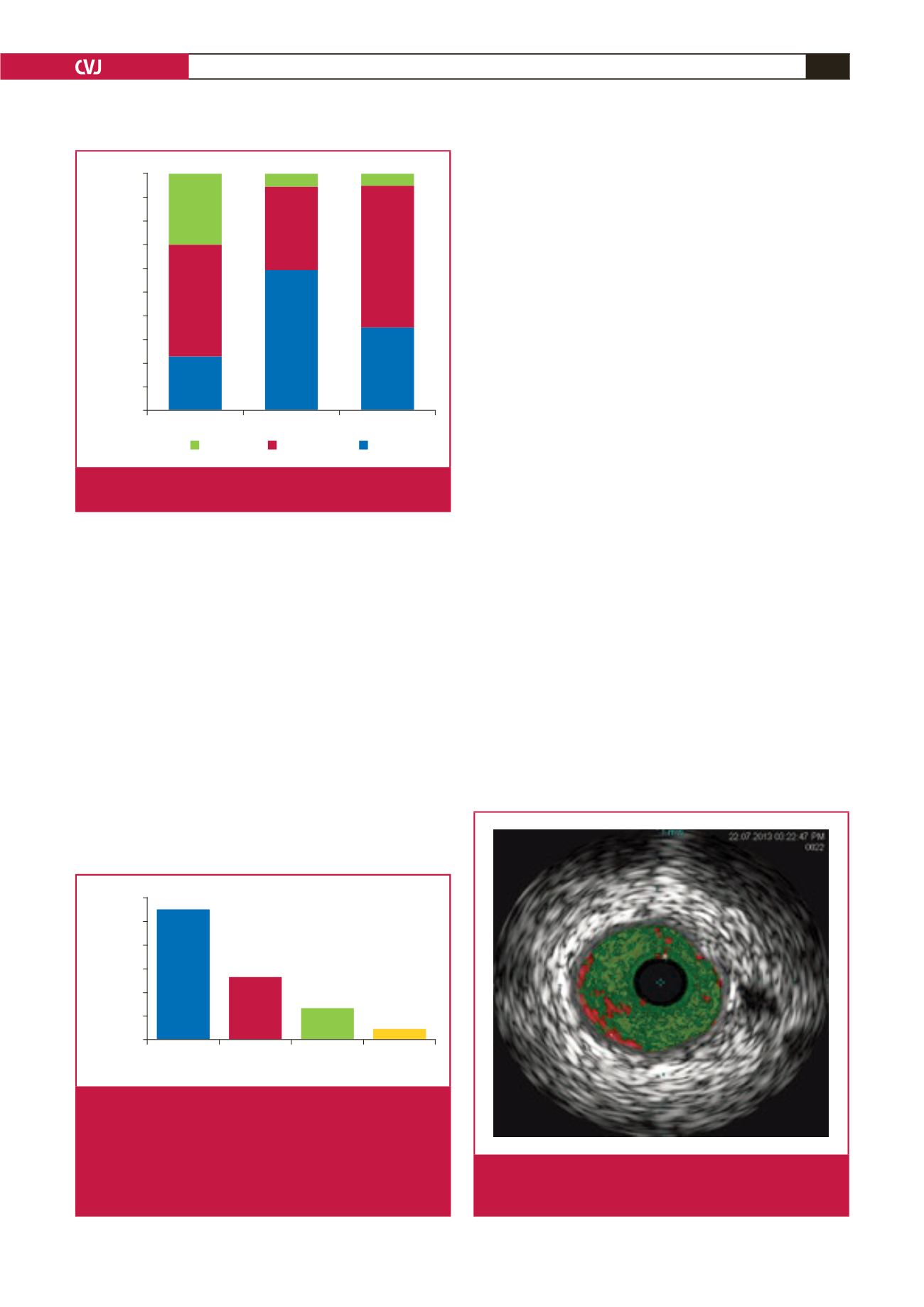
coronary vasculature was of moderate degree, while in 35% the
total plaque burden was mild, and in a minority (5%) it was
severe (Fig. 1). The atherosclerotic disease was significantly
higher in the proximal coronary vasculature compared to the
mid and distal segments of the coronary arteries (
p
=
0.010).
Furthermore, it was significantly higher in the mid segments
than in the distal segments of the coronary arteries (
p
=
0.0006).
There was more severe plaque burden (30%) in the culprit vessel
compared to non-culprit vessels (5%).
Assessment of the entire coronary vasculature by VH in these
patients demonstrated that the predominant plaque morphology
consisted of fibrous plaque (55.4%). Fibro-fatty plaque was
found in 26.6% of patients, necrotic core was present in 13.3%,
and dense calcium was present in only 4.7% of patients (Fig. 2).
There were significant differences between the mean volumes
of fibrous plaque, fibro-fatty plaque, necrotic core and dense
calcium (all
p
<
0.05).
On assessing plaque morphology in the culprit coronary
arteries, the major plaque morphology remained fibrous plaque
(56.5%), while fibro-fatty tissue (21.2%), necrotic core (14.4%)
and dense calcium (3.6%) plaque constituted the remainder (Fig.
2). In non-culprit arteries, the lesion morphology was similar,
with fibrous plaque found in 55.1% of patients, fibro-fatty
plaque in 29.5%, necrotic core in 8.2% and dense calcium in 4.8%
of patients.
Discussion
This was a prospective study using VH-IVUS to characterise
the coronary plaque morphology in HIV-positive patients
presenting with ACS. First, we demonstrated that some form of
atherosclerosis was present in all HIV-positive patients presenting
with ACS without any prior cardiac history. Even normal vessels
on angiography were found to have atherosclerosis, and in 5%
of these vessels, the plaque burden was surprisingly severe.
Our findings help explain the discrepancy of lower plaque
volumes that have been reported in HIV-positive patients studied
angiographically, as coronary angiograms are not accurate in
defining minor plaque volumes.
15
Second, our study has shown that the predominant plaque
morphology in the coronary arteries of HIV-positive patients
presenting with ACS consisted of fibrous tissue in just over
half of all patients and fibro-fatty tissue in a further quarter
of patients. Necrotic core lesions were uncommon and dense
calcified lesions were rare. Hence the plaque morphology
in HIV-positive patients can be described as predominantly
non-calcified fibrous and fibro-fatty disease (Fig. 3).
Our findings are supported by non-invasive imaging such as
coronary computer tomography angiography (CCTA), which
has shown an increased prevalence of subclinical atherosclerosis
in HIV-positive compared with HIV-negative patients.
16,17
A
recent meta-analysis of 1 229 asymptomatic HIV-positive
patients on cART demonstrated a three-fold higher prevalence
Culprit
Non-culprit
Total
Percentage plaque
100
90
80
70
60
50
40
30
20
10
0
Severe
30
34
5
5
60
47
Moderate
Mild
Fig. 1.
Plaque burden in HIV-positive patients with acute
coronary syndrome.
Fibrous
tissue
Fibro-fatty
tissue
Necrotic
core
Dense
calcium
Percentage plaque
60
50
40
30
20
10
0
Fig. 2.
Virtual histology in HIV-positive patients with acute
coronary syndrome. The mean fibrous plaque volume
was significantly greater than the mean fibro-fatty
plaque volume, which was significantly greater than
the mean necrotic core volume. This in turn was
significantly greater than the mean dense calcium
volume (all
p
<
0.05).
Fig. 3.
Virtual histology intravascular ultrasound of non-calci-
fied fibrous and fibro-fatty plaque from HIV-positive
patients with acute coronary syndrome.