


















 9 / 64
9 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 3, May/June 2020
AFRICA
117
excretion of liquids and electrolytes is increased, together
with suppression of levels of the fluid-regulating hormones
renin, angiotensin II, aldosterone and arginine vasopressin to
control plasma volume,
21,22
and peripheral vascular resistance is
decreased.
23-25
Several studies have established the effectiveness of planned
interventions using physical exercise in the treatment of HTN
with land and aquatic-based exercises,
26-33
but comparisons
between the two types of exercise regarding elderly hypertensives
trained in different modalities are scarce. In addition, the effects
on PEH of land- and aquatic-based exercise during the following
24 hours need further investigation.
In light of the benefits of AE, this study compared resting
BP using ambulatory BP monitoring (ABPM), the clinical gold-
standard methodology for assessing BP status, in two groups
of trained subjects with equivalent cardiorespiratory capacity
performing either LE or AE. In addition, using ABPM, we
assessed PEH after AE and LE among older women with HTN.
Methods
This was a controlled clinical trial developed at the Exercise
Physiology Laboratory (LABFE) of the school of Physical
Education of Ouro Preto, Minas Gerais, Brazil. The study
protocol was approved by the Research Ethics Committee
of the Federal University of Ouro Preto under protocol:
38383314.3.0000.5150.
The study population consisted of 40 elderly hypertensive
women, 20 trained in land-based exercise and 20 in aquatic-based
exercise. To be included, the subjects had to meet the following
criteria: aged over 60 years, hypertensive, female, in regular
treatment for BP control, and enrolled in recurrent physical
exercise for at least six months before evaluation for a minimum
of twice a week. Subjects with symptomatic cardiorespiratory
disease or cardiac alterations, the metabolic syndrome, renal or
hepatic disease, cognitive impairment, and any other medical
contra-indications of physical exercise were excluded.
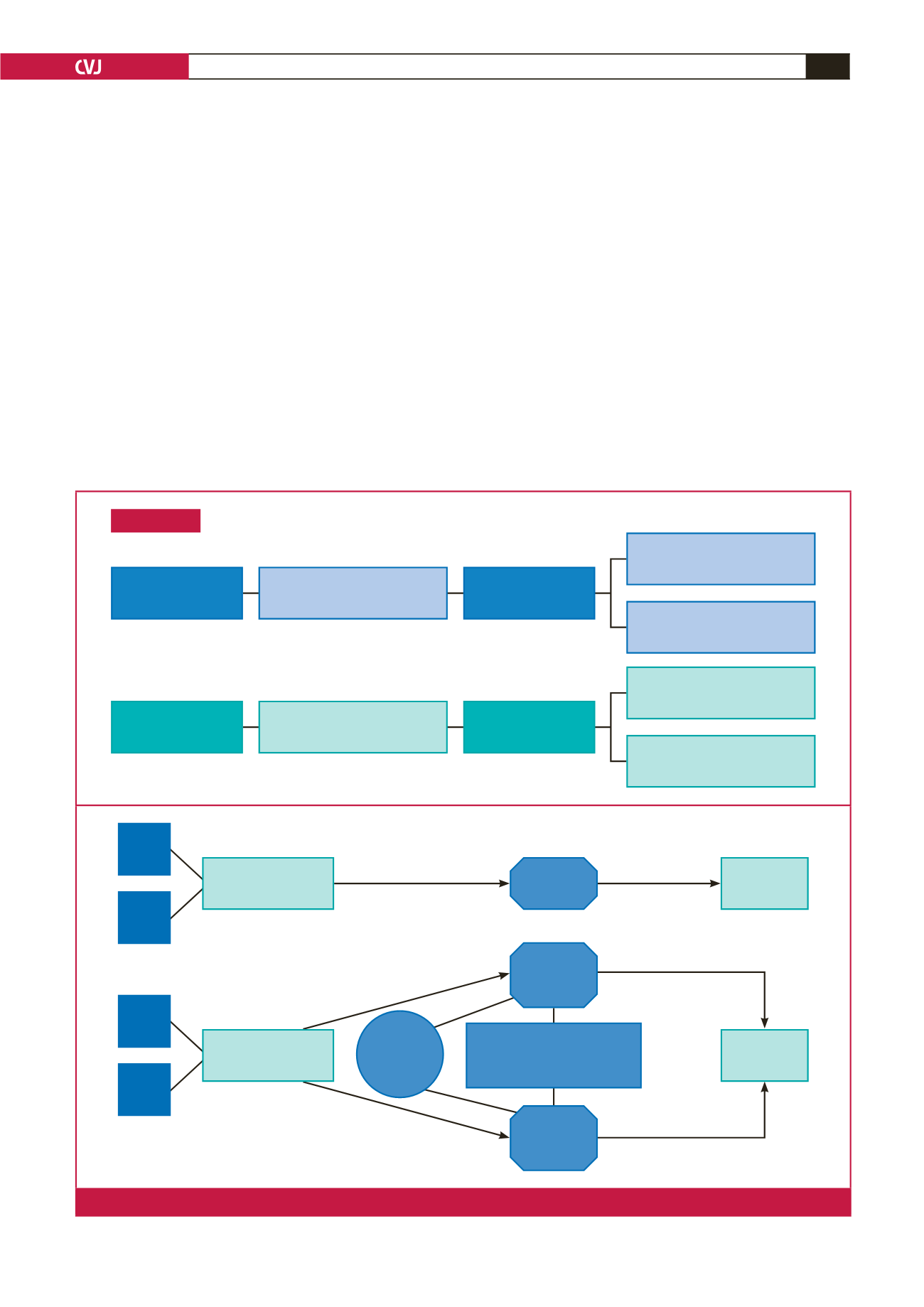
The participants were divided randomly into four groups:
Enrollment
Assessed for eligibility
in aquatic exercise
(
n
= 27)
Assessed for eligibility
in land exercise
(
n
= 33)
Excluded (
n
= 7)
Not meeting inclusion criteria (
n
= 4)
Declined to participate (
n
= 3)
Excluded (
n
= 13)
Not meeting inclusion criteria (
n
= 7)
Declined to participate (
n
= 6)
Baseline aquatic training effects
(AE) (
n
= 10)
Baseline land training effects
(LE) (
n
= 10)
Aquatic exercise hypotension effect
(AE-PEH) (
n
= 10)
Land exercise hypotension effect
(LE-PEH) (
n
= 10)
Randomised
(
n
= 20)
Randomised
(
n
= 20)
AE
AE-PEH
LE
LE-PEH
Evaluation
cardiopulmonary test
ABPM
24 h
ABPM
24 h
Rest of 48 h
75% RHR
50 minutes
Aquatic envi-
ronment
75% HRR
50 minutes
land environ-
ment
3 BP meas-
ures before
exercise RHR
Evaluation
cardiopulmonary test
5 minutes: preparatory activity
20 minutes: aerobic exercise
20 minutes: resistance exercise
5 minutes: stretching exercise
Fig. 1.
Study design. RHR: reserve heart rate; ABPM: ambulatory blood pressure measurement.