


















 31 / 62
31 / 62

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 4, July/August 2020
AFRICA
193
548 BP measurements (median of four per patient) showed that
increase in BP over a median follow up of 2.3 years (IQR: 1.5–2.6)
was associated with established risk factors for hypertension,
and that there was no evidence of an independent deleterious
effect of any class of anti-retroviral drugs on BP.
23
We therefore
recommend studies to unveil the effects in highly prevalent areas
for hypertension, such as the case of Mozambique.
24
A high prevalence of RHD (30.4/1 000) has been reported
in schoolchildren from the geographical area where the
study was undertaken.
5
Researchers in Uganda suggested a
possible protective role of HIV infection in modulating RHD
susceptibility. Borderline/definite RHD prevalence of 0.82%
(95% CI: 0.26–2.23%) was found on echocardiographic screening
of HIV-infected children, a low prevalence compared to the
1.5–4% prevalence among Ugandan children.
25
In Africa, anaemia has been linked to recurrent episodes
of malaria, tropical splenomegaly, parasitic intestinal disease,
among other infectious and nutritional causes. Because it is
the most common adverse effect of ART
26,27
and frequently
occurs independent of HIV infection,
28
moderate to severe
anaemia is often left untreated; this was the case in our cohort.
Several anaemic patients were found without any treatment,
despite levels of haemoglobin well below the internationally
recommended cut-off points.
We advocate that anaemia should be considered a risk factor
for several cardiovascular conditions affecting HIV patients,
including heart failure and cardiomyopathy.
29
It has been linked
to poorer virological suppression in Uganda.
30
Without targeted
measures for its correction, it persists in a considerable proportion
of patients after 12 months of ART.
31
More importantly, the
resolution of HIV-related anaemia has been proven to improve
quality of life, physical functioning, energy and fatigue.
16
Systolic and diastolic dysfunction were common in
paucisymptomatic HIV-infected patients. A meta-analysis by
Cerrato
et al
., to appraise the incidence of cardiac dysfunction in
HIV-infected paucisymptomatic individuals, performed a pooled
analysis of 2 242 patients from 11 studies.
32
An overall average
incidence of systolic and diastolic left ventricular dysfunction
of 8.3% (95% CI: 2.20–14.25) and 43.4% (95% CI: 31.73–55.03),
respectively, was found. Hypertension (OR = 2.30; 95% CI:
1.20–4.50) and older age (OR = 2.50 per 10 years’ increase; 95%
CI: 1.70–3.60) were predictors of LV diastolic dysfunction.
32
Themortality rate of 2.4%at two years occurred predominantly
in patients with cardiovascular disease (four out of six). It could
have been prevented by surgery (RHD and CHD), indicating
the need for efforts to invest in improving access to diagnosis
and management of chronic cardiovascular diseases in endemic
areas for HIV in Africa. Also, we performed a follow-up
ultrasound for 14.2% of patients (44/252) at 24 months. We were
able to determine the vital status and confirm the absence of
symptomatic heart failure for all participants at five years, by
medical visits, consultation of their hospital files and phone calls.
At the five-year follow up there were 24 (9.5%) deaths.
Programmes by non-physicians
33,34
to screen for cardiac
disease have shown that non-specialists can perform focused
cardiac ultrasound and use algorithms for risk stratification
and management. We believe that, supported by robust referral
systems to ensure that high-risk patients reach specialist care,
these task-shifting strategies should be considered for under-
resourced areas in sub-Saharan Africa because of their potential
to maximise the gains obtained with the dissemination of ART.
HIV infection in older people occurs concomitantly with some
cardiovascular risk factors and may require multidisciplinary
care.
35
Our results not only corroborate the association of HIV
and ART with cardiometabolic traits in sub-Saharan Africa,
36
but also support systematic cardiovascular screening in younger
people on ART. Furthermore, owing to the mounting evidence
showing that countries with a high burden of HIV also have
an increased burden of non-communicable diseases such as
hypertension,
37
economic implications on the already under-
resourced health systems in Africa need to be considered.
Conclusions
Cardiovascular risk and disease was evident in HIV-infected
individuals in a cohort of relatively young patients on long-
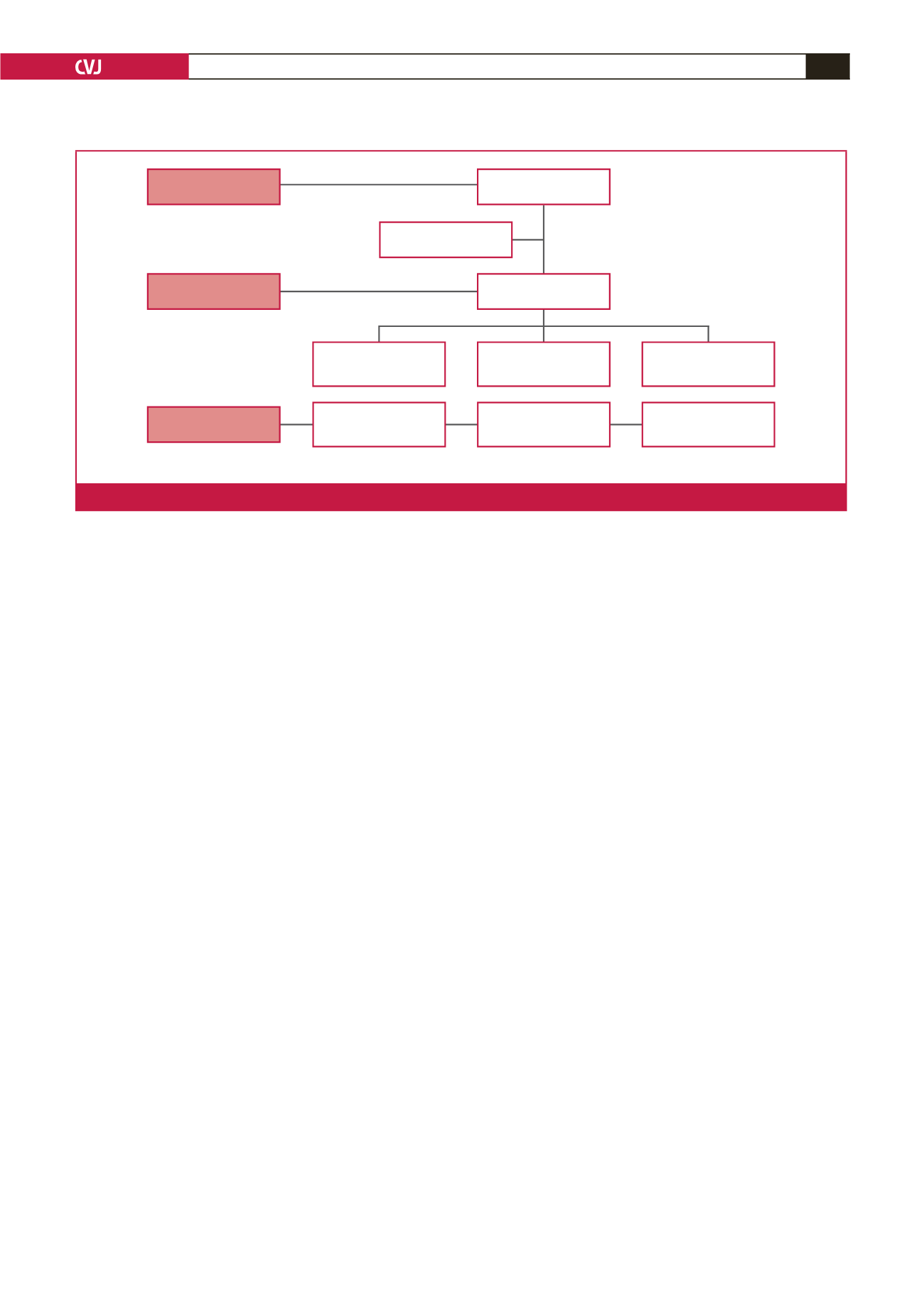
US – cardiac ultrasound
264 recruited
12 did not have US
252 with US
Lost to follow-up 3
(1.2%)
Lost to follow-up 5
(2.1%)
6 deaths
(2.4%)
220 with follow-up
(90.5%)
243 with US
(96.4%)
Deaths 18
(7.4%)
Baseline
24-month follow-up
5-year follow-up
Fig. 1.
Flowchart of the study.