CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 4, May 2013
e2
AFRICA
Surgical correction of the anomalous coronary artery was
proposed to the patient but she refused surgery. Therefore, the
patient was discharged on medical therapy with the advice to
avoid strenuous physical activity.
Discussion
Abnormalities of the coronary arteries can be reported in
approximately 0.3 to 1% of the population. Because these
abnormalities are usually not associated with other congenital
cardiac malformations, patients do not show any clinical
manifestations and have a good prognosis.
2
A systematic classification of abnormalities of the coronary
tree has been obtained by imaging techniques.
2-5
Specifically,
coronary angiography performed in patients with atherosclerotic
disease have obtained an ‘invasive’ evaluation of these coronary
anomalies.
3,4
Alternatively, these abnormalities have been studied
by a ‘semi-invasive’ imaging technique, such as transoesophageal
echocardiography.
5
In the last few years, non-invasive imaging techniques such as
MSCT have allowed physicians to obtain a clear reconstruction
of the coronary tree.
6
In patients in which coronary angiography
gives a clear picture of the coronary anatomy, MSCT usually
does not add any further information. On the other hand, in
those cases in which coronary arteries are not clearly visualised
by angiography, MSCT is a significant help. Specifically, this
technique is extremely sensitive in demonstrating atherosclerosis
of the coronary arteries and it is very useful in the evaluation of
coronary artery stenosis in individuals without known coronary
artery disease.
7,8
Moreover, MSCT use in the coronary intervention laboratory
has recently increased because this technique may help in
evaluating the length of coronary occlusion, the calibre of the
distal vessel and the presence of distal disease. This information
could have a pivotal role in driving the interventional strategy
before PCI.
9
Advantages and disadvantages of CT over conventional
angiography are still debated. As reported above, the main value
of MSTC seems to rule out only ‘significant’ coronary artery
disease and it is almost as good as coronary angiography for
detecting true false-positives. On the other hand, it seems to
be poorer in its rate of false-positives.
10
Therefore, although
it is a highly effective non-invasive alternative to coronary
angiography for the exclusion of obstructive coronary artery
stenosis, it is likely that it will still require coronary angiography
for MSTC positives, partly to identify MSCT false-positives, but
also because angiography provides other information that CT
currently does not. Specifically, details of the insertion site and
distal run-off for possible coronary artery bypass graft.
10
Moreover, the diagnostic accuracy varies at the individual
artery level, because results are slightly worse for the LAD and
CX arteries compared with the RC and LM arteries. Another
important issue to bear in mind is that patients undergoing
MSCT are exposed to higher radiation doses compared with
invasive coronary angiography. This has resulted in concerns
being raised about repetitive use of 64-slice CT or its use in
younger individuals or women of childbearing age.
11
In the present report, we described a clinical case in which
coronary angiography did not permit us to fully elucidate
whether the RCA and LAD originated separately or not.
Unfortunately, the patient’s clinical conditions did not permit us
to perform MSCT before PCI, therefore the culprit lesion of the
proximal RCA was acutely treated with PCI. This choice arose
A
C
B
D
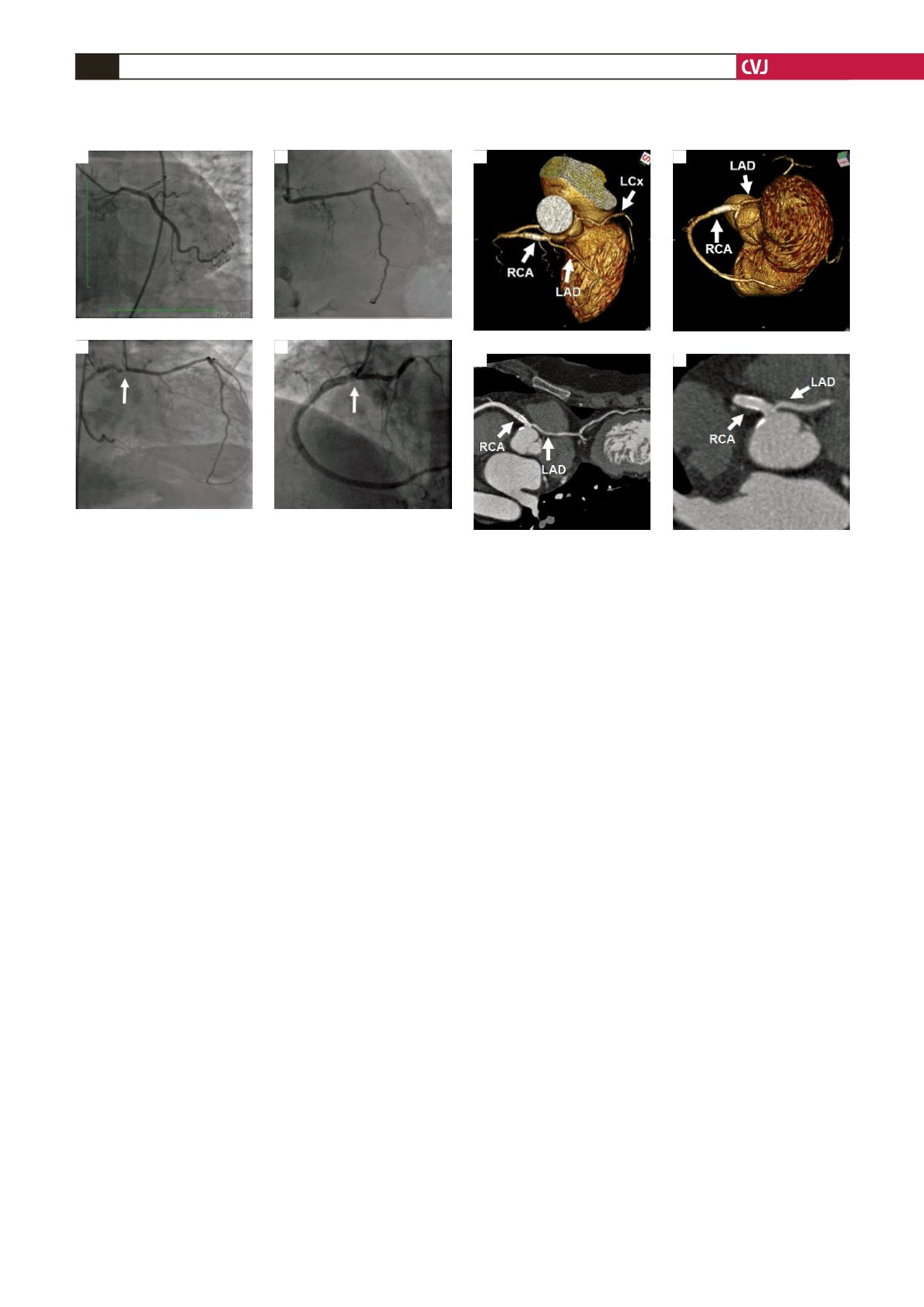
Fig. 1. Coronary angiograms showing the coronary anat-
omy. A: The left circumflex artery (LCx) originated from
the left sinus of Valsalva. B: The right coronary artery
(RCA) and left anterior descending artery (LAD) originat-
ed from the right sinus of Valsalva. Arrow indicates the
stenosis of the proximal RCA. C: Final result after stent
implantation. Note the complete visualisation of both the
RCA and LAD.
Fig. 2. Multi-slice computed tomography imaging (MSTC)
and 3D coloured volume rendering of the coronary arter-
ies. A and B: Three dimensional reconstruction of the
coronary arteries shows the RCA and LAD sharing a
very short common coronary vessel before continuing
separately. C and D: Contrast-enhanced 64-slice CT coro-
nary angiography indicates that the stent in the RCA is
perfectly implanted and that it does not obstruct the LAD.
A
C
B
D


