CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 4, July/August 2014
e2
AFRICA
on the same antibiotic regimen targeted to a completion of a
six-week course before any surgical action would be taken.
By the end of the fourth week of conservative treatment, the
patient unexpectedly went into cardiac arrest and immediate
cardiac resuscitation was instituted. Cardiac function was
restored an hour later and the patient was transferred to the
intensive care unit (ICU). Due to her critical condition, after
initial haemodynamic stabilisation with appropriate inotropic
support, the patient was able to undergo surgery three days later.
At operation, the aortic valve appeared severely damaged
with two of the cusps (left, non-coronary) bearing vegetations
and perforations. Two small vegetations were also found and
removed from the anterior leaflet of the mitral valve. The
aortic valve was replaced with a pulmonary autograft (Ross
procedure) while the right ventricular outflow tract (RVOT)
was reconstructed with a 14-mm bovine jugular vein conduit
(Contegra
®
, Medtronic Inc, Minneapolis MN, USA).
The patient made an uneventful recovery. Cultures of valve
and vegetations were positive for
Aspergillus
. After a further
four weeks of appropriate intravenous antibiotic and antifungal
treatment, the patient was discharged home in excellent clinical
condition with negative blood cultures.
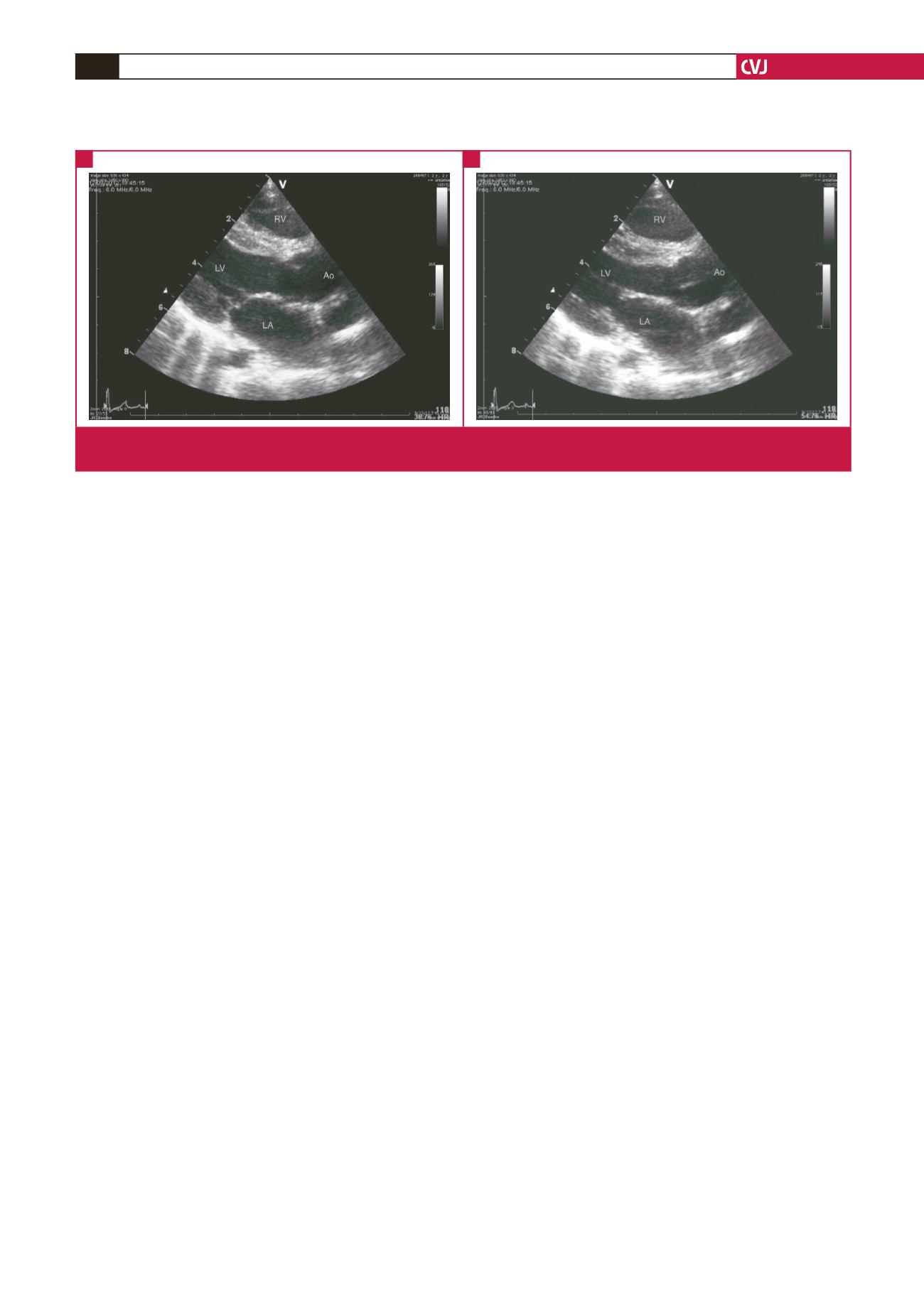
One year later, both the neo-aortic and the implanted
xenograft in the pulmonary position were found to perform well,
without stenosis or regurgitation (Fig. 2). The patient remained
in an excellent clinical condition and continued to receive oral
antifungal prophylaxis.
Discussion
Despite the increase in number of documented reports of fungal
endocarditis in children, bacterial endocarditis remains more
common.
Aspergillus
is a rare cause of endocarditis, usually
affecting immunosuppressed children younger than a year of
age, and premature neonates.
1
Mortality rate is high and the
commonly negative blood cultures render diagnosis elusive, the
latter not infrequently established on post mortem.
2
While searching for the ideal prosthesis for replacement of
the aortic valve in children, the pulmonary autograft transfer,
first described by DN Ross, has emerged as an attractive
option.
3
Advantages include lack of immunological degenerative
changes, freedom from anticoagulation, excellent haemodynamic
performance, and potential for growth.
4-8
The need for simultaneous RVOT reconstruction has been
met by the extensive use of aortic and pulmonary cryopreserved
homografts.
9,10
Alternatively, the Contegra
®
valved conduit is
also well suited for RVOT reconstruction without the use of
additional foreign material, remaining well functioning without
calcification during early and medium follow up.
11,12
Although technically demanding, the Ross procedure has
been recommended as the procedure of choice for aortic
valve replacement in children, with excellent operative, short-
and medium-term results.
4,13-15
Nonetheless, concern has been
expressed about the long-term durability of the neo-aortic valve
as the need for re-operation increases with time due to late
dilation and valve insufficiency.
6,7
Although aortic homograft
root replacement has been described as a reliable option for
acute aortic valve endocarditis in children, the Ross procedure
has been successfully performed with minimal mortality and
recurrence rate.
16,17
Conclusion
Aspergillus
endocarditis may occur even in immunologically
healthy young children in the setting of structural cardiac
pathology. The Ross procedure proves to be a reliable option
for surgical treatment of acute aortic endocarditis and can be
performed whenever indicated owing to commercially available
bioprosthetic valved conduits.
References
1.
Millar BC, Jugo J, Moore JE. Fungal endocarditis in neonates and chil-
dren.
Pediatr Cardiol
2005;
26
: 517–536.
2.
Challa S, Prayaga AK, Vemu L, Sadasivan J, Jagarlapudi MKM,
Digumarti R, Prabhala. Fungal endocarditis: an autopsy study.
Asian
Cardiovasc Thorac Ann
2004;
12
: 95–98.
3.
Gonzalez-Lavin L, Geens M, Ross DN. Pulmonary valve autograft for
aortic valve replacement.
J Thorac Cardiovasc Surg
1970;
60
: 322–330.
4.
Raja SG, Pozzi M. Ross operation in children and young adults: the
Fig. 2.
Postoperative parastenal long-axis view with the neo-aortic valve open (A) and closed (B). A thin, well-functioning neo-aortic
valve is depicted.
A
B


