
















 21 / 78
21 / 78

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 4, July/August 2015
AFRICA
167
three months were treated with anti-arrhythmics (amiodarone in
three cases and propofenone in one case).
Regular follow up consisted of out-patient clinic visits one,
three and six months after the procedure. It included a detailed
history for arrhythmia-related symptoms (palpitations, chest
discomfort, fatigue and dizziness), a physical examination,
12-lead ECG and 24-hour Holter monitoring.
The need for further oral anticoagulation was evaluated in the
third month based on the CHA
2
DS
2
-VASc score. Outcome was
measured as per the guidelines in the recent consensus document.
6
Any episode of AF, atrial flutter, or atrial tachycardia lasting for
at least 30 seconds was defined as recurrence.
6
A blanking period
was not considered for the study. Any recurrence in the first three
months was classified as early recurrence, whereas recurrence
after this period was considered late recurrence. Only patients
with at least six-month follow ups were included in the study.
Patients with late AF recurrence underwent redo-procedures
to evaluate the cause of recurrence, following similar preparatory
steps to those during the index procedure. A diagnostic catheter
was used to evaluate the status of isolation or reconnection in
each vein.
None of the patients had clinical signs of coronary ischaemic
episodes either prior to or at the end of the procedure. There
were no changes in the ST-segment when comparing ECG
tracings before, during and after the procedure.
Statistical analysis
SPSS 17.0 software (IBM Corp, Armonk, NY, USA) was used
for statistical analysis. All quantitative variables with a normal
distribution were reported as mean
±
standard deviation, and
compared using the Student’s
t
-test. For values with non-normal
distribution, comparison was performed with the Mann–
Whitney
U
-test. For the descriptive variables comparison, the
Pearson
χ
2
or Fisher’s exact tests were used, when appropriate.
The independent association of clinical variables with
recurrence was assessed using multivariable linear regression.
A Kaplan–Meier analysis was used to analyse the recurrent
atrial tachycardia‐free survival after cryo-ablation. A
p
-value
<
0.05 was considered statistically significant. Receiver-operator
characteristic (ROC) analysis was performed on significant
predictors to calculate the accuracy and other diagnostic
parameters, and to determine a cut-off point at the maximum
sum of sensitivity and specificity.
Results
Baseline characteristics and demographic features of the patients
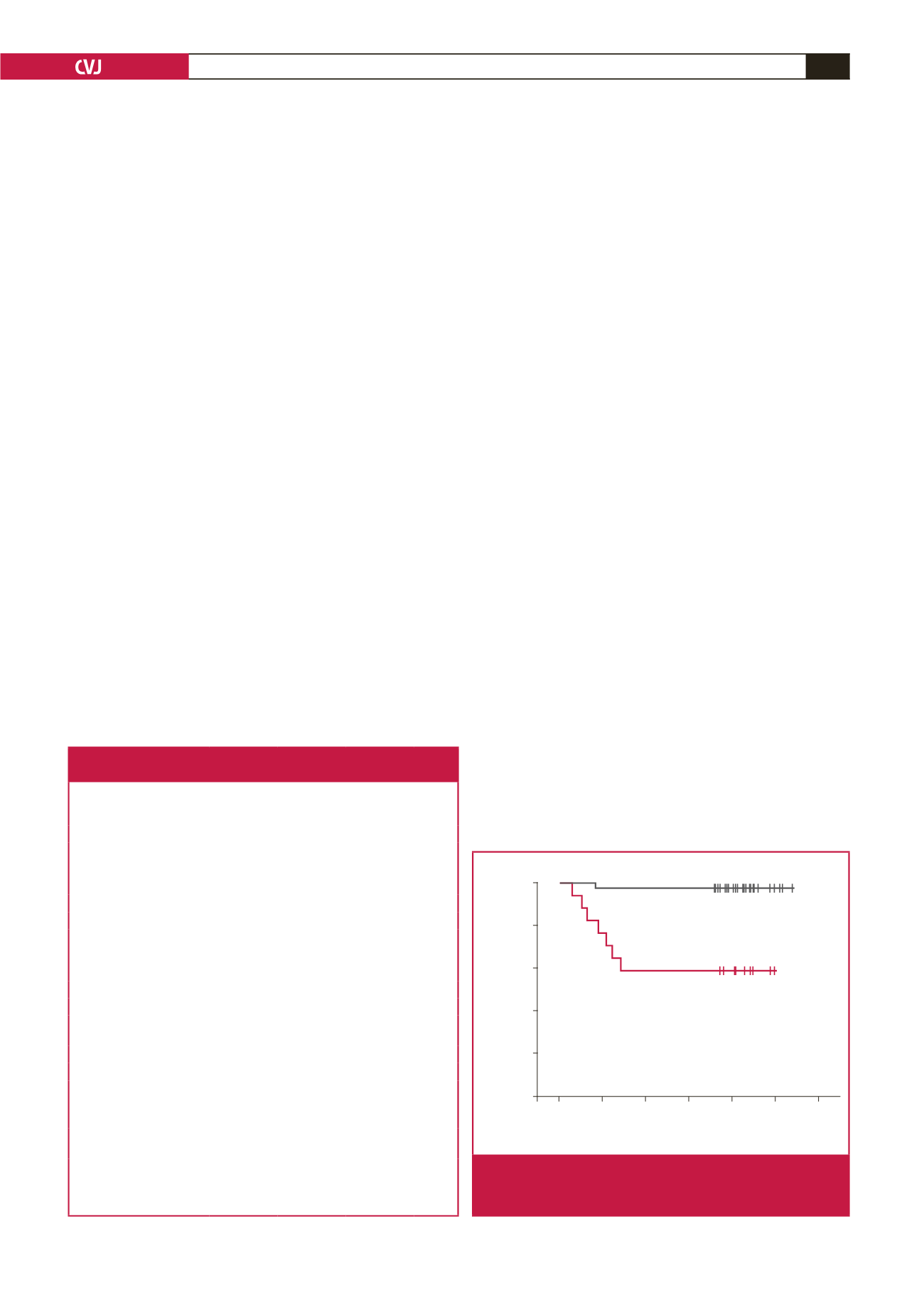
are presented in Table 2. After a mean follow-up period of 214
±
24 days (range 180–274), early recurrence was observed in five
(8.77%) patients and late recurrence in two (3.50%) (Fig. 1).
Patients with AF recurrence (group 1) were significantly older
(65
±
15 vs 54
±
1 years,
p
=
0.002), had larger left atrial diameters
(46.2
±
4.3 vs 40.7
±
4.1 mm,
p
=
0.002) and longer duration of
AF (6.7
±
4.5 vs 3.5
±
1.9 years,
p
=
0.002) than patients with
no recurrence (group 2). The other baseline demographics were
comparable between the groups.
All patients were in sinus rhythm at the beginning of the
procedure. The procedural endpoint of PVI was reached in all
patients. A left-sided common ostium was seen in two patients.
Four patients were in AF at the end of cryo-ablation; the regions
of CFE were located within the PV antrum or posterior LA
wall in these four patients, and additionally on the LA roof in
three patients, and high on the LA septum in one patient. Sinus
rhythm was achieved in all four patients after CFE ablation.
At the end of CFE ablation, repeat induction was attempted in
all four patients but neither AF nor atrial tachyarrhythmia was
induced after CFE ablation in any of them.
Mean procedure time and mean duration of energy delivery
were comparable in the groups, but mean minimal temperature
Table 2. Baseline characteristics and demographic features of the
study population (
n
=
57)
Total
(
n
=
57)
Recurrence
(
–
)
(
n
=
50)
Recurrence
(+)
(
n
=
7)
p-
value
Failed anti-arrhythmics (
n
)
Amiodarone
13
11
2
0.630
Propofenone
27
23
4
0.594
β
b or CKB
17
15
2
0.409
Age, years (mean
±
SD)
55.1
±
12.13 54
±
1
65
±
15 0.021
Gender, female,
n
(%)
29 (50)
26 (52)
3 (42)
0.658
BMI, kg/m
2
24.8
±
3.7 24.8
±
3.6 24.7
±
3.7 0.126
Diabetes mellitus,
n
(%)
10 (17)
9 (18)
1 (14)
0.195
Hypertension,
n
(%)
25 (43)
21 (42)
4 (57)
0.451
CAD,
n
(%)
9 (15)
8 (16)
1 (14)
0.457
Smoking,
n
(%)
28 (49)
25 (50)
3 (42)
0.702
Duration of AF history,
years
3.9
±
2.6 3.5
±
2.5 6.7
±
4.5 0.002
LA diameter, mm
41.32
±
4.51 40.72
±
4.16 46.23
±
4.36 0.002
LVEF, %
59.23
±
5.12 59.48
±
4.78 56.42
±
5.56 0.146
CHA
2
DS
2
-VASc score,
mean
±
SD
1.3
±
1.17 1.3
±
1.11 1.7
±
1.60 0.414
EHRA score, mean
±
SD 2.45
±
0.56 2.44
±
0.54 2.57
±
0.78 0.573
Follow-up time, days,
mean
±
SD
214
±
24 212
±
23 213
±
25 0.117
AF, atrial fibrillation;
β
b, beta-blocker; BMI, body mass index; CKB, Ca
channel blocker; CAD, coronary artery disease; EHRA, European Heart
Rhythm Association; LA, left atrium; LVEF, left ventricular ejection fraction;
SD, standard deviation,
p
<
0.05.
>8 censored
1–8 censored
>8
1–8
1.0
0.8
0.6
0.4
0.2
0.0
0 50 100 150 200 250 300
Follow up (months)
Freddom from AF recurrence
Fig. 1.
A Kaplan–Meier analysis was used to analyse the
recurrent atrial tachycardia‐free survival after cryo-
ablation in the troponin group.