
















 51 / 78
51 / 78

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 4, July/August 2015
AFRICA
197
The echocardiogram demonstrated a severely dilated right
ventricle, free PR and a RVOT peak instantaneous gradient
(PIG) of 60 mmHg. After successful pre-stenting of the RVOT,
a Melody
®
valve was successfully implanted using a 22-mm
Ensemble
®
system (see Methods). No residual PS or PR was
demonstrated post valve implantation.
Case 2
The second case was a 16-year-old female (weight 50.0 kg) with
double-outlet right ventricle (DORV) and pulmonary stenosis.
She had had a DORV correction and a 20-mm aortic homograft
insertion at the age of 12 years. RVOT rehabilitation was
indicated due to a mixed lesion of PS and PR.
Echocardiography demonstrated a calcified RVOT with a
PIG of 52 mmHg and a dilated right ventricle with moderate to
severe PR. Coronary artery anatomy was favourable. A 22-mm
Ensemble
®
delivery system was used to successfully implant a
Melody
®
valve (see Methods). The right ventricle pressure was
reduced with no residual PR.
Case 3
The patient was a 31-year-old male (weight 47.5 kg) with DORV
and pulmonary stenosis. He had had RVOT reconstruction with
a 21-mm homograft at age 17 years. Surgery was considered risky
due to a direct retrosternal location of the original homograft
(Figs 2, 3). His main indication for re-valvulation was pulmonary
stenosis with a RVOT PIG of 60 mmHg.
A stable ‘landing site’ was constructed using two stents and
pre-dilation with a high-pressure balloon (see Methods). The
Melody
®
valve was then delivered using an 18-mm Ensemble
®
delivery system. The valve was dilated using a high-pressure
balloon and a good result was achieved. The patient did well
with mild transient retrosternal chest pain as the only complaint.
Methods
Valve implantation was performed under general anaesthesia. All
patients were heparanised following our standard protocol, and
prophylactic antibiotics (Cefazolin) were given. Vascular access
was obtained via the femoral vessels and haemodynamic data
were collected pre and post Melody
®
valve implantation (Table 1).
Simultaneous coronary angiography and inflation of a
low-pressure balloon (Amplatzer
TM
sizing balloon II, St Jude
Medical, St Paul, MN, USA) in the RVOT was performed
to exclude coronary artery occlusion (Fig. 4).There were no
coronary artery occlusions or ECG changes detected during
balloon inflation, and the decision was made to continue with
the procedure.
Preparing the landing zone for Melody
®
valve implantation
is a crucial step in the procedure. It is important to record any
stent recoil during balloon deflation. A stiff guide wire [Meier
(Boston Scientific, Natick, MA, USA), Lunderquist
TM
extra stiff
(Cook Medical, Bloomington, USA)] with stable position was
obtained. In our experience, pre-stenting of the RVOT is more
challenging and once the landing site is prepared, the Melody
®
valve is implanted with minimal difficulty.
Table 1. Haemodynamic information
RV pressure
(mmHg)
MPA pressure
(mmHg)
PR
pre
post
pre
post
pre
post
Case 1
35/6
32/6
20/7
20/8
severe
none
Case 2
74/6
42/6 52/13
32/17
severe
none
Case 3
56/6
34/6 24/6
24/9
moderate
none
RV: right ventricle; MPA: main pulmonary artery pressure; PR:
pulmonary regurgitation.
Fig. 2.
CT angiography. The homograft (large arrow) in case 3
is positioned anterior and to the right of the aorta (ao).
Note the direct retrosternal position of the calcified
homograft. The coronary arteries (small arrows) are
at low risk for compression during valve implantation.
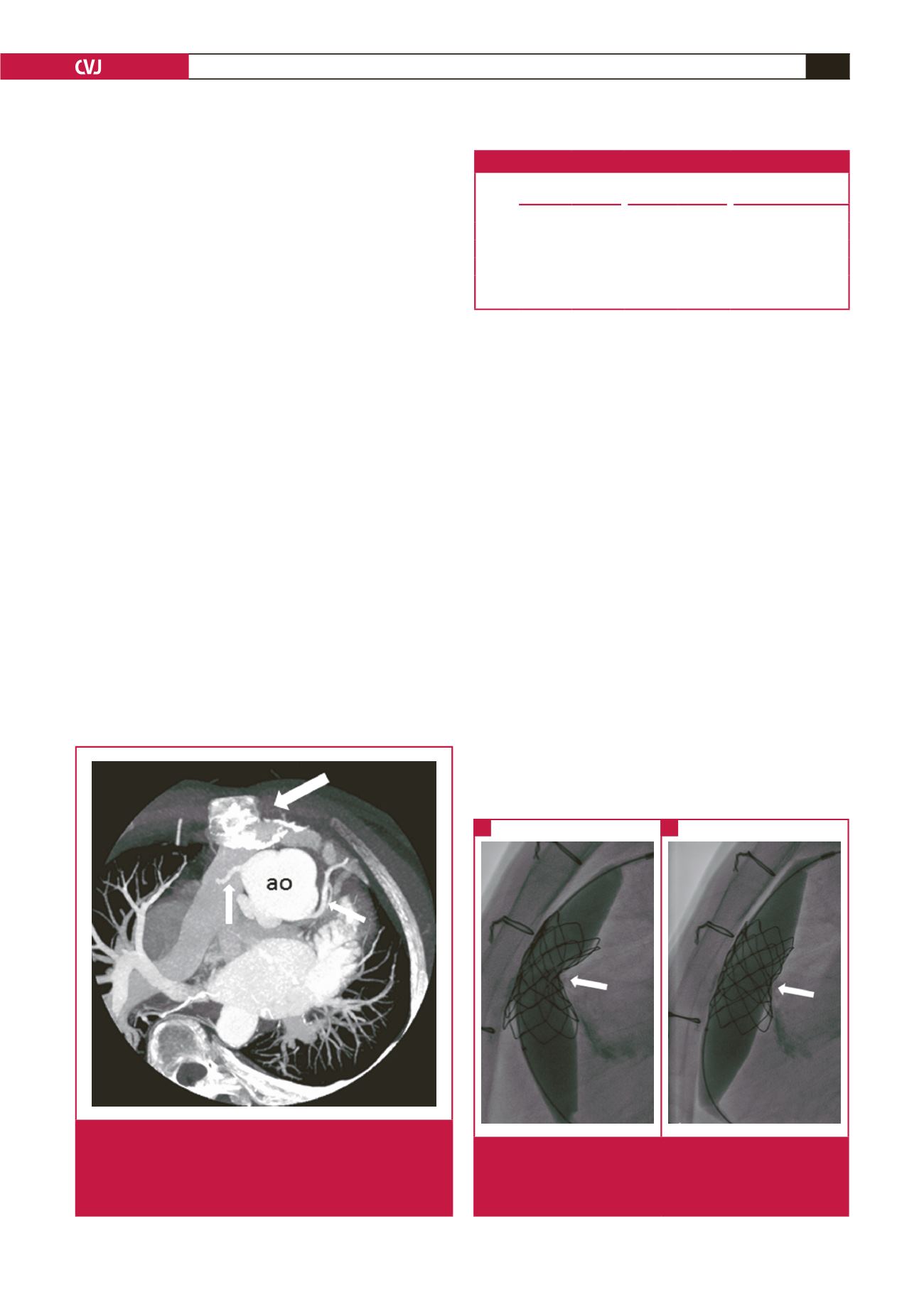
Fig. 3.
Direct retrosternal position of the stenotic RVOT with
inflation of a high-pressure balloon (Atlas
®
PTA dilata-
tion catheter, Bard Medical). The arrows indicate stent
indentation pre and post dilatation (Case 3).
A
B