
















 68 / 70
68 / 70

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 5, September/October 2016
e6
AFRICA
was the case in our patient.
EMF can be associated with parasitic infestations and
their attendant eosinophilia. An association with
Schistosoma
mansoni
,
haematobium
and
intercalatum
has been reported.
4-6
In
the our case,
Schistosoma
infection may have been the trigger
for clinical aggravation due to the superimposition of Loeffler’s
syndrome on chronic fibrotic EMF. Although we found no
calcification or other signs of chronic schistosomiasis, we cannot
exclude previous episodes.
Conclusion
Our findings support the hypothesis of EMF being a progressive
disease that may be linked to repetitive inflammatory insults,
which may correspond with successive episodes of blood
and endomyocardial hypereosinophilia triggered by parasitic
infestation or other factors. They also suggest the need to
explore new management approaches, including prevention of
recurrences in patients with chronic, established disease. This
should probably involve strict control of endemic parasitic
infections, as well as the use of anti-inflammatory drugs and
anticoagulants, mimicking the current standard of care in
Loeffler’s syndrome. The EMF diagnosis and scoring system
previously used in community screening, considering only the
severity and distribution of structural lesions,
2
could probably
be improved to include inflammation, cardiac and coagulation
biomarkers, thereby allowing its use for risk stratification and
tailored management of this neglected cardiomyopathy.
References
1.
Mocumbi AO, Yacoub S, Yacoub MH. Neglected tropical cardiomyo-
pathies: II. Endomyocardial fibrosis: myocardial disease.
Heart
2008;
94
(3): 384–390.
2.
Mocumbi AO, Ferreira MB, Sidi D, Yacoub MH. A population study of
endomyocardial fibrosis in a rural area of Mozambique.
N Engl J Med
2008;
359
(1): 43–49.
3.
Andy JJ, Ogunowo PO, Akpan NA,
et al
. Helminth associated hypere-
osinophilia and tropical endomyocardial fibrosis (EMF) in Nigeria.
Acta Trop
1998;
69
(2): 127–140.
4.
Carneiro RC, Santos AL, Brant LC,
et al.
Endomyocardial fibrosis
associated with mansoni schistosomiasis.
Rev Soc Bras Med Trop
2011;
44
: 644–645.
5.
Assimeng J, Segbefia CI, Neequaye J. Endomyocardial fibrosis associ-
ated with
Schistosoma haematobium
infection.
Ghana Med J
2014;
48
(4):
225–227.
6.
Bustinduy AL, Luzinda K, Mpoya S,
et al
. Endomyocardial fibrosis
(EMF) in a Ugandan child with advanced hepatosplenic schistoso-
miasis: coincidence or connection?
Am J Trop Med Hyg
2014;
91
(4):
798–800.
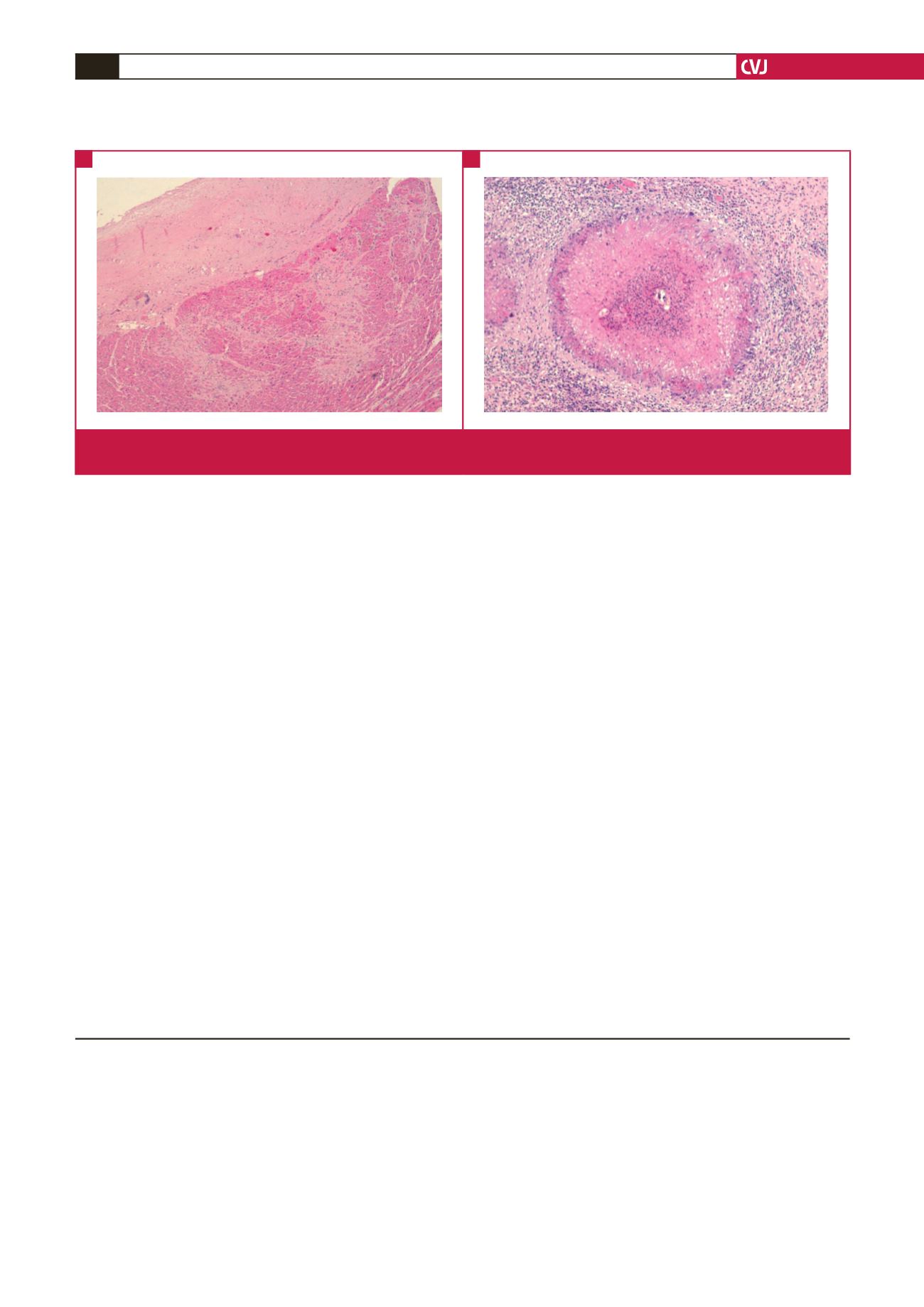
Fig. 2.
Histological features of EMF include endocardial thickening by fibrosis, with strands of fibrous tissue penetrating the inner
myocardium (A). Eosinophilic granulomas centred by viable
Schistosoma
eggs were found in the bladder (B).
A
B