
















 17 / 80
17 / 80

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 3, May/June 2017
AFRICA
151
Madagascar. This was particularly for hypertensive subjects,
female participants and semi-urban dwellers. The overall
prevalence of the MS was lower than reported in Ghana among
hypertensive patients. It was however similarly observed that the
MS was more prevalent among women than men (OR: 4.88,
p
=
0.027) in this study.
17
Another study among newly diagnosed
type 2 diabetes subjects revealed higher prevalences of the MS
of 68 and 81%, using IDF and WHO criteria, respectively.
Again, as in our study, the MS was common in women and was
driven essentially by female gender, family history of diabetes,
overweight and obesity.
18
IFG overall prevalence was 9.3% and ranged from 15.3% in
Cameroon to 4.0% in Nigeria. Our findings are however higher
than reported in a community-based study in South Africa,
19
and Nigeria.
20
These differences could be accounted for by the
differences in study types (hospital based vs community based)
and also geographical variations in the populations studied.
However, the high prevalence of IFG among the participants is
significant, as this represents a group of individuals at increased
risk for transition to higher cardiovascular risk and the eventual
development of diabetes if not properly controlled with lifestyle
and dietary modifications.
Recent publications have highlighted the rapidly increasing
prevalence of hypertension, coupled with under-diagnosis, under-
treatment and low control rates in SSA.
4,20,21
The high prevalence
of hypertension in our hospital-based study and the fact that
25.8% of these patients were newly diagnosed or undiagnosed
cases is therefore not surprising. The situation was similar with
diabetes mellitus, with an overall prevalence of 15.7%, with 6.9%
being undiagnosed cases, as previously described.
22
In a recent meta-analysis that focused on the burden of
hypertension in Africa,
4
the pooled prevalence was 30%. Our
prevalence is equivalent to the highest prevalence of 70% in
the pooled studies. Another recent population-based study in
Cameroon
21
reported a prevalence of 47.5%, which was lower
than reported in our cohort.
TheCLARIFYregistry,whichexploredgeographicalvariations
in cardiovascular risk factors among coronary artery disease
(CAD) patients, reported a high prevalence of hypertension of
48% in Eastern Europe.
23
The differences observed in these studies
and others could be due to differences in populations studied and
methodologies employed. Previous regional-based studies using
similar methodology to ours are non-existent, therefore limiting
the possibility for adequate comparison.
The high prevalence of diabetes in our study (15.7%) was
slightly below the 17% noted among CAD patients in Eastern
Europe but far lower than the 60% in the Middle East.
23
While we acknowledge the dearth of African regional data on
diabetes, some national studies are worth noting. The highest
prevalence of diabetes among participating countries was from
Nigeria, with a prevalence rate of 24.8%. This was lower than
the 28.2% noted in a community-based study in South Africa,
19
but higher than the 10.1% reported in a self-selected population
study in Cameroon.
22
Variations in degree of urbanisation, and
differences in lifestyle, environmental factors and study settings
(population vs hospital based) as well as sample sizes most likely
account for the differences seen in these studies.
Overall mean BMI of our study participants was 28.5 kg/m
2
,
which was higher than reported in Benin,
8
although it was lower
than reported in Ghana among hypertensive subjects.
17
About
one in three of the study participants was overweight or obese.
This is likely to be explained by the increasing adoption of
Western lifestyles, especially in urban areas (which were in the
majority in our study), limited physical activity and increased
sedentary lifestyles, which are wrongly attributed to good living.
Similarly, a high prevalence of obesity has been reported in
other parts of Africa,
8,17,24
in relation to urbanisation and high
socio-economic status.
25
A community-based study in Cameroon
by Fezeu and colleagues in 2010 demonstrated the influence of
ethnicity and urbanisation on abdominal adiposity and obesity-
related abnormalities.
26
A quarter of participants reported excessive alcohol
consumption, and approximately one in five was either a current
or former smoker. This is similar to the 19% smoking prevalence
reported in Eastern Europe.
23
These are well-established drivers
for CVD,
27
metabolic and other NCDs and most likely account in
part for the high rates of hypertension, diabetes and obesity in our
cohort. Our findings are supported by a recent meta-analysis of
prospective studies on the association of alcohol consumption and
CVD risk and mortality, where it was found that low-to-moderate
alcohol consumption was inversely significantly associated with the
risk of CVD and all-cause mortality among hypertensive patients.
27
Risk profiles of the participants were examined according
to hypertension status. A high prevalence of diabetes (17.7%)
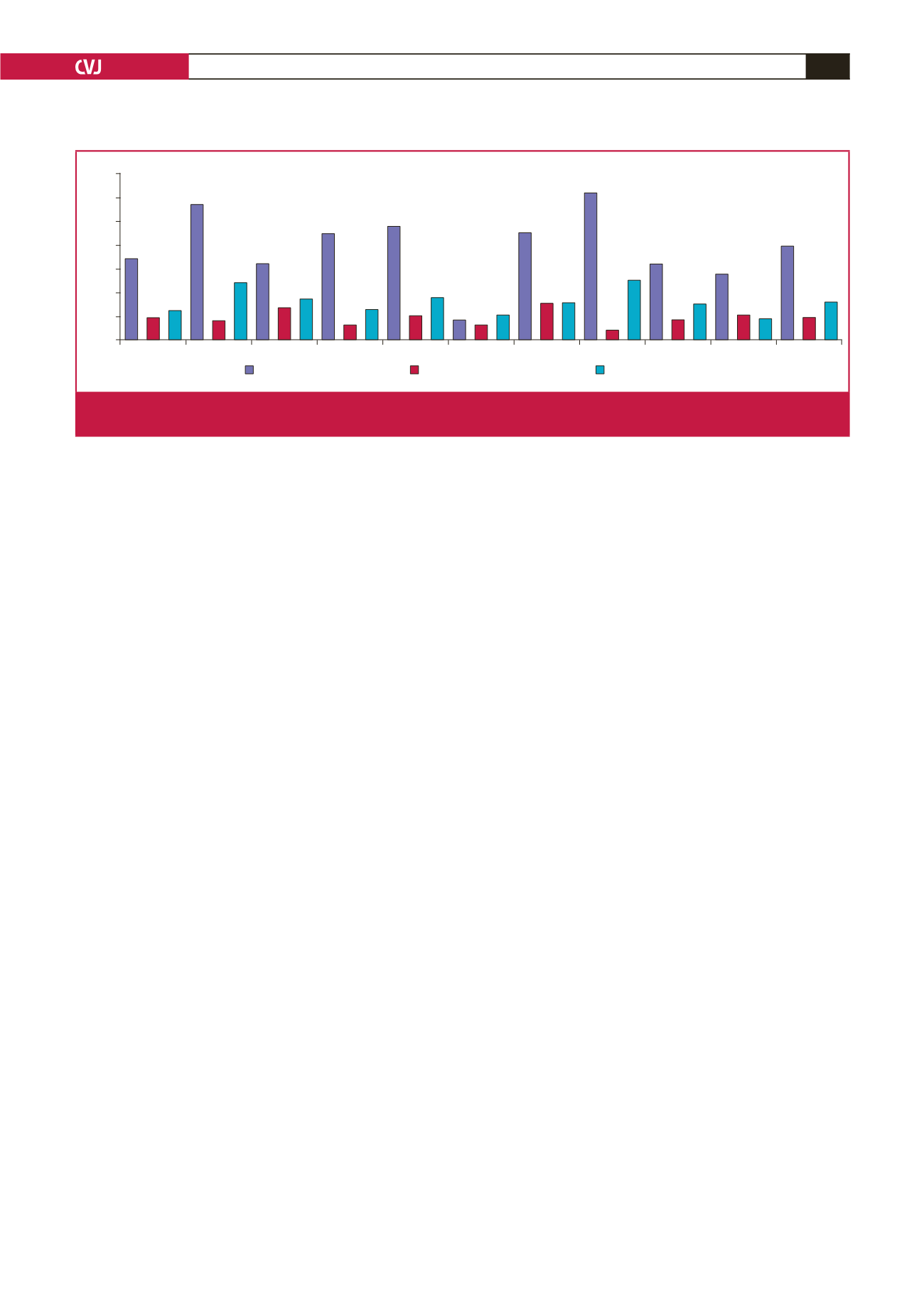
Urban Semi-urban Males Females
HTN N-HTN Cameroon Nigeria
DRC Madagascar
Total
70
60
50
40
30
20
10
0
Impaired fasting glucose
Metabolic syndrome
Diabetes mellitus
Percentage (%)
34.3
57
32.1
44.7
47.8
8.3
45.2
62.1
31.9
27.7
39.4
9.3
8.1
13.6
6.2
10.1
6.2
15.3
4
8.3
10.4
9.3
12.3
24.1
17.2
12.7
17.7
10.4
15.6
24.8
15
8.7
15.7
Fig. 1.
Prevalence of the metabolic syndrome, impaired fasting glucose levels and diabetes across countries, urbanicity, gender and
hypertension status. HTN = hypertensives, N-HTN = non-hypertensives