
















 15 / 82
15 / 82

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 1, January/February 2018
AFRICA
13
layered aortic tissue, then through the graft, using continuous
4/0 prolene sutures without pledgetted sutures or band. In those
undergoing aortic root replacements, adequate native aortic
tissue was left in the non-coronary sinus area, allowing eversion,
while the anastomosis in the right and left coronary sinus area
was performed with reinforcement from a Teflon band, since
there was insufficient aortic tissue to allow for eversion.
After proximal aortic anastomosis, the coronary arteries were
anastomosed to the graft by eversion of the excess aortic tissue in
the button (Fig. 1). Subsequently, cardioplegia was administered
through a needle over the graft to check bleeding at the proximal
anastomosis line and the coronary implantation suture lines
(Fig. 2). A clamp was then placed on the innominate artery and
the cross-clamp was removed. The aortic tissue was everted to
accomplish the distal anastomosis of the graft under antegrade
cerebral perfusion and mild hypothermia.
In patients with additional cardiac pathologies, aortic
replacement was completed after the surgical procedure for the
cardiac pathology had been carried out. In patients undergoing
aortic root replacement with a valved conduit, a modified
Bentall procedure with flanged graft was used, as we believe
that this approach may help reduce the risk of tissue–prosthesis
incompatibility as well as the risk of bleeding, in addition to
shortening the duration of anastomosis.
5
When simultaneous
coronary bypass surgery was done, proximal anastomoses were
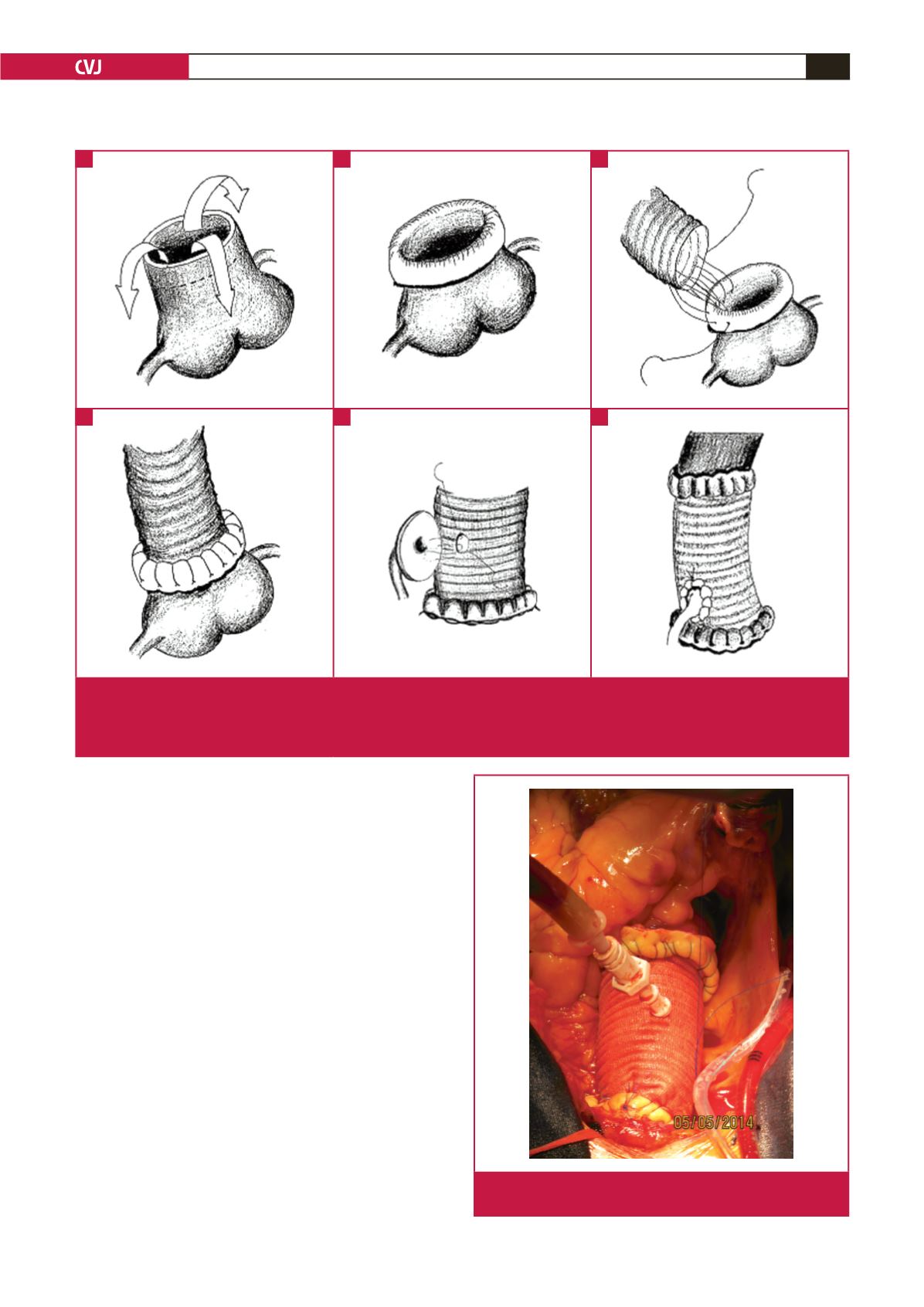
Fig. 1.
A: We left 2 cm of aortic tissue to allow for eversion of the aorta. B: Double-layered aortic tissue is prepared by everting and
suturing 2 cm of aortic tissue. C: Proximal anastomosis is performed using continuous 4/0 prolene sutures. D: View of the
ascending aorta after proximal anastomosis. E: In the aortic root replacement, double-layered aortic tissue is prepared at
the coronary buttons. F: View of the aorta after coronary anastomosis.
A
D
B
E
C
F
Fig. 2.
Control of bleeding with administration of cardioplegia
via a needle over the graft.