
















 19 / 82
19 / 82

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 1, January/February 2018
AFRICA
17
320-detector row CT scanner, rest CCTA was performed without
stress CCTA.
7
A further study performed both stress and rest
CCTA scans with a 320-detector row CT scanner,
9
but the rest
CCTA scan was followed by a stress CCTA scan. All of these
studies used invasive FFR as the reference standard.
Invasive FFR is a well-established and highly accurate
method for assessing the functional significance of coronary
artery stenosis; however, it is limited by its invasive nature.
Stress perfusion CMR is a well-established and highly accurate
non-invasive method used to assess the functional significance of
coronary artery stenosis. Therefore, we designed a study protocol
based on CCTA using a wide detector in which a stress scan was
followed by a rest scan, and stress perfusion CMR was used as a
reference standard.
The aim of this study was to determine whether TAG could be
valid for detecting haemodynamically significant coronary artery
stenosis using wide-area detector CT, compared to the reference
standard of stress perfusion CMR as a reference standard.
Methods
This prospective study was approved by the institutional review
board. Informed consent was obtained from all subjects prior
to examination. From May 2012 to January 2015, all patients
with moderate coronary artery stenosis (50–70%) detected on
invasive coronary angiography (ICA), who were required to
undergo haemodynamic significance testing were enrolled, and
underwent adenosine stress CCTA and stress perfusion CMR.
Exclusion criteria included a history of coronary artery bypass
graft surgery or other cardiac surgery, myocardial infarction
(MI) or heart failure, atrial fibrillation, second- or third-degree
atrioventricular block, impaired renal function, symptomatic
asthma, pregnancy or any contra-indications to iodinated
contrast agents, or other any MR imaging contra-indication.
Stress CCTA protocol
All patients were scanned on a wide-area detector CT scanner
(Aquilion ONE, Toshiba Medical System, Otawara, Japan) with
320-detector rows (each 0.5-mm wide) and a gantry rotation time
of 350 ms. The entire heart was imaged in a single heart beat with
a maximum of 16-cm coverage in the Z direction.
After intravenous adenosine infusion (140
µ
g/kg/min for
three minutes; Denosin injection 90 mg/30 ml; BC World Pharm
Co, Ltd, Seoul, Korea), stress CCTA was performed using the
biphasic injection method (Fig. 1). A 60-ml bolus of iodinate
contrast (lobitridol, Xenetics 350; Guerbet, Paris, France) was
injected intravenously, followed by a 50-ml saline chaser at a
flow rate of 5 ml/s. To identify the optimal phase of contrast
enhancement for adenosine stress CCTA, we performed a
10-second dynamic scan 15 seconds after initiating contrast
injection.
10
All scans used prospective electrocardiogram (ECG)
gating that covered phases 30–50% of the R-R interval.
Rest CCTA was performed 10 min after adenosine stress
CCTA. The rest scan was acquired during the injection of 50 ml
of iodinate contrast, followed by 50 ml of saline at a flow rate
of 5.0 ml/s. The phase window was set at 30–50% of the R-R
interval in patients with a heart rate (HR)
≥
75 beats per minute
(bpm), and 65–85% of the R-R interval in patients with a HR
<
75 bpm. For most cases, prospective ECG gating covering
65–85% of the R-R interval was used.
Stress perfusion CMR protocol
CMR was performed using a 3.0-T unit (Magnetom Skyra;
Siemens, Erlangen, Germany) with an 18-channel body coil.
The imaging protocol consisted of three parts: ciné imaging for
ventricular volume and function; first-pass contrast-enhanced
myocardial perfusion imaging during adenosine-induced
stress and under resting conditions; and myocardial delayed
enhancement imaging.
For the perfusion study, adenosine was injected as described
for the CCTA protocol, after which 0.05 mmol/kg of gadolinium-
based contrast material (gadoterate meglumine, Dotarem;
Guerbet, Villepinte, France) was injected intravenously at an
injection rate of 3 ml/s, followed by a 25-ml saline flush. First-
pass stress myocardial perfusion imaging of three short-axis
imaging planes positioned in the base, mid and apical myocardial
segments of the left ventricle was performed using a saturation-
recovery turbo-fast low-angle shot (FLASH) gradient echo
sequence. Fifteen minutes after stress perfusion imaging, rest
perfusion images were acquired after a second bolus of 0.1
mmol/kg gadolinium-based contrast was injected.
Analysis of CCTA and CMR imaging
Adenosine stress CCTA data and stress perfusion CMR images
were reviewed by two experienced readers (six and 16 years of
experience with CCTA and CMR), blinded to the ICA results.
Three major coronary arteries per patient were evaluated. TAG
was manually obtained for each vessel using an image post-
processing workstation (Vitrea 6.4; Vital Images, A Toshiba
Medical Systems Group, Minnetonka, MN, USA), following the
method described by Wong
et al
.
7
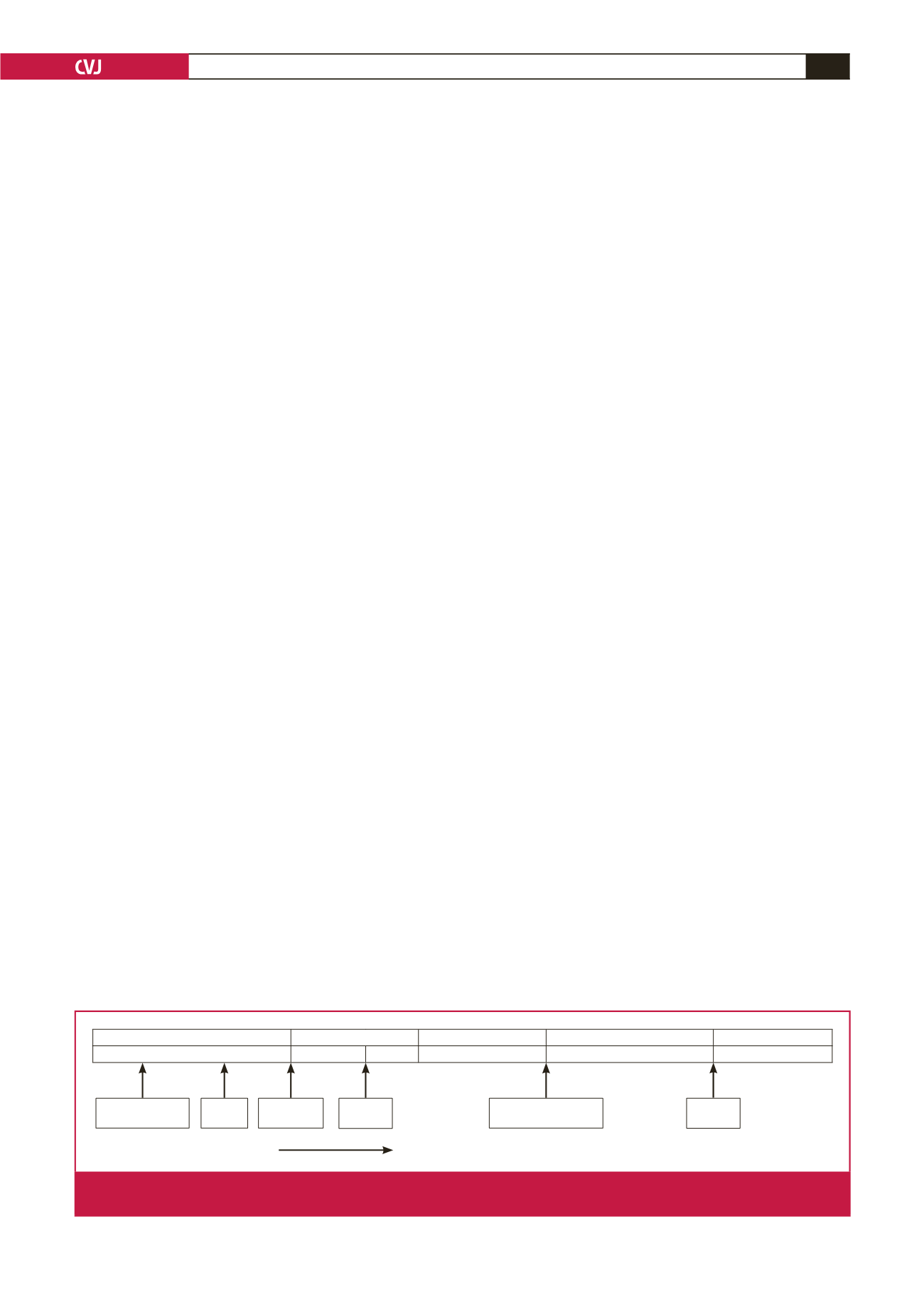
Beta blockade,
ECG monitoring
Adenosine
infusion
Adenosine infusion
ceased
IV
contrast
IV
contrast
Scout
images
Pre-scan
3 min
Dynamic stress scan Waiting for HR to baseline
Rest scan
2 min 45 sec 15 sec
10 sec
10 min
Coronary CTA
Time
Fig. 1.
CCTA protocol. After a 3-min intravenous adenosine infusion, contrast-enhanced stress CCTA was acquired, followed by a
rest CCTA after 10 minutes. CCTA
=
coronary computed tomography angiography.