
















 77 / 82
77 / 82

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 1, January/February 2018
AFRICA
e11
with cuffing of the aortic knob. The ECG (Fig. 2) at our
unit showed a normal sinus rhythm, normal QRS axis with
sub-epicardial ischaemia in the inferior and apico-lateral leads.
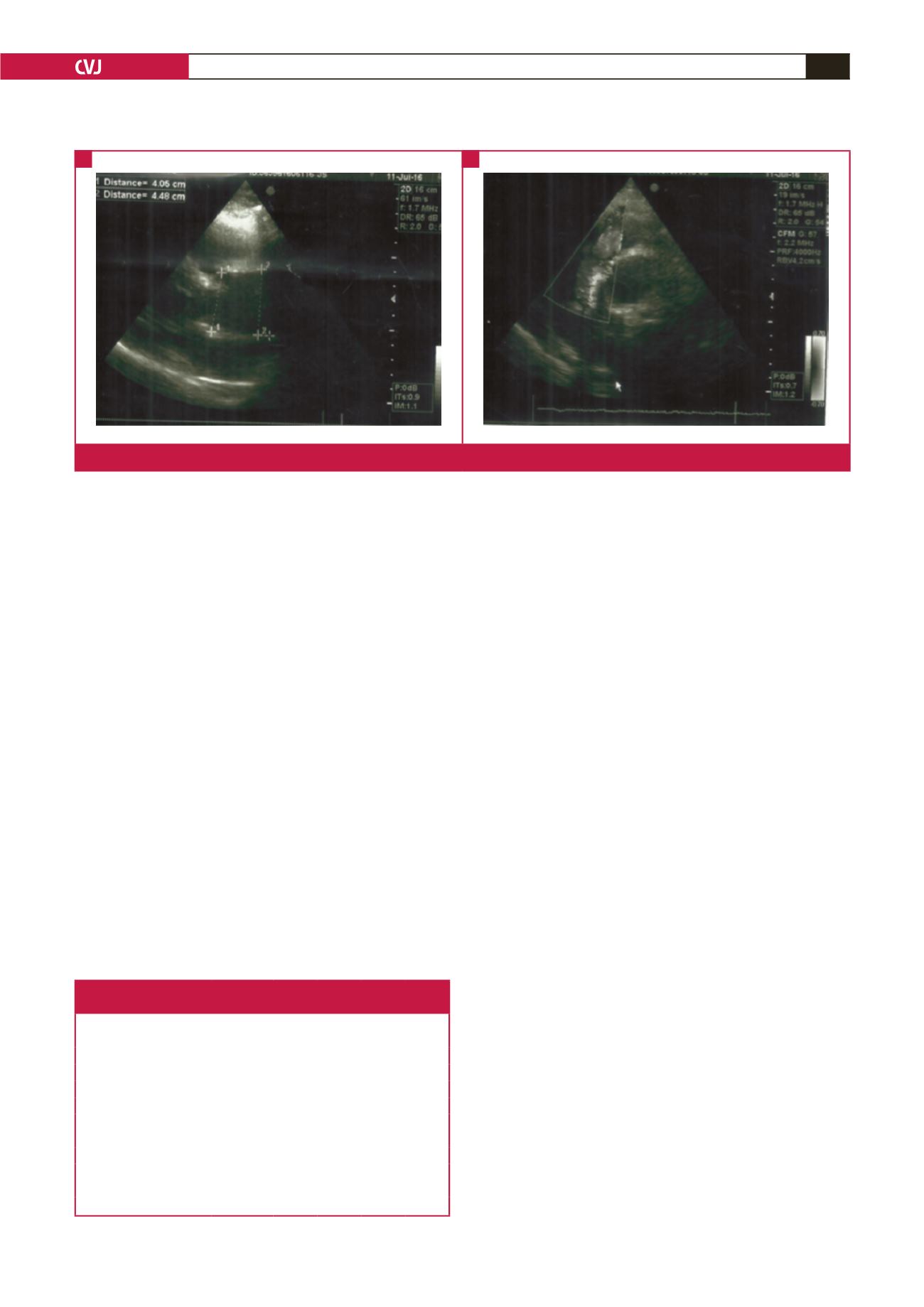
Echocardiography (Fig. 3) showed a dilated left atrium, good
left ventricular systolic function (ejection fraction 72%), and
severe aortic insufficiency with dilatation of the aortic root and
ascending aorta (44 mm).
Contrast-enhanced CT (CECT) angiogram of the thorax
(Fig. 4) showed dissection of the aorta from the ascending aorta
to the iliac arteries, including the coeliac trunk and left renal
artery, and causing splenic infarction. Doppler ultrasound of
the carotid arteries did not show extension to the carotid arteries.
These observations led to a working diagnosis of Standford type
A acute aortic dissection. Table 2 shows biological investigations
done at presentation and throughout hospitalisation.
The patient was placed on high-flow oxygen at 5 l/min,
nicardipine in an electric syringe titrated to a maximum of 10
mg/h, bisoprolol 5 mg/12 h, analgesics and compressive stockings.
The LMWH was stopped. On day five of hospitalisation, he
developed superficial thrombophlebitis on the left forearm (along
the peripheral intravenous line). By day six of hospitalisation,
blood pressure and heart rate targets (
<
120/80 mmHg and
<
60
beats/min, respectively) were achieved.
On day 10 of hospitalisation, the patient developed a
temperature of 39.1°C and sudden dyspnoea at rest. Physical
examination showed a heart rate of 119 beats/min, blood
pressure of 124/76 mmHg and oxygen saturation of 98%. Chest
examination revealed crepitation in both lung bases, more
marked on the right. We decided on a presumptive diagnosis
of severe pneumonia. A repeat chest X-ray (Fig. 1B) showed
bilateral interstitial heterogeneous opacities.
The C-reactive protein (CRP) level was 310.43 mg/l with
leucocytosis of 17.7
×
10
6
cells/l (Table 2). Blood samples were
collected for culture, and antibiotics (amoxicillin–clavulanic
acid 1 g eight hourly and clarithromycin 1 000 mg 12 hourly)
were introduced. Blood culture results (which returned after the
patient’s demise) were positive for
Klebsiella pneumonia.
About
three hours later he had persistent dyspnoea and hypoxaemia
(SpO
2
≤
65% and PaO
2
≤
60 mmHg). He was intubated and
during the process sustained a cardiac arrest. The patient later
died on day 12 of hospitalisation following cardiopulmonary
arrest despite life support.
Discussion
AAD is characterised by separation of the layers of the aortic
wall, resulting from the entry of extra-luminal blood through
an intimal tear, producing a false lumen. Tears are commonly
seen at areas of high stress, commonly in the anterior aortic wall
just above the aortic valve (66%) and the posterior wall of the
proximal descending aorta (33%). When blood enters through
an intimal tear it passes longitudinally along the tunica media
separating the intima from the adventitia.
13
There are several
different classification systems of aortic dissection. The two
most commonly used formats are the DeBakey and Standford
classifications, as described in literature.
12,14
The typical presentation of AAD is a sudden, unexpected,
intense retrosternal pain radiating to the back and/or abdomen,
associated with asymmetrical blood pressure.
6
Patients are
typically hypertensive, middle aged or elderly and therefore the
differential diagnosis would include acute myocardial infarction,
acute coronary syndromes, pericarditis, pulmonary embolism,
peptic ulcer disease and acute pancreatitis. Due to its possibility
of extension to involve the mesenteric, iliac and renal arteries,
other presentations may include intestinal ischaemia, stroke and
Table 2. Serial biological investigations done at the emergency
department and throughout hospitalisation
Biological investigation
Presentation Day 1 Day 4 Day 10 Day 11
White cell count,
×
10
6
cells/l
6.8
9.5
7.3
5.2
17.7
C-reactive protein, mg/l
<
6
7.21 30.72 310.43 ND
Haemoglobin, g/l
15.2
13.5 13.2 12.4 10.5
Serum creatinine, mg/l
17.2
12.3 ND 13.1 ND
Troponin I
2.26
0.69 ND ND 0.15
Creatine kinase (CK), IU/l
200
ND ND ND ND
CK-MB, IU/l
24.9
ND ND ND ND
LDH, UI/l
455
ND ND ND ND
D-dimers
24087
ND ND ND ND
NT-pro BNP
117
ND ND ND 6,366
LDH = lactate dehydrogenase test; ND = not done.
Fig. 3.
Echocardiography showing dilatation of the ascending aorta.
A
B