


















 12 / 64
12 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 6, November/December 2020
292
AFRICA
temperature > 37.5°C and/or being vaccinated or donating
blood within three months prior to participation. Additionally,
we excluded participants with missing values of NT-proBNP
(
n
= 12), resulting in 397 participants (194 Africans and 203
Caucasians).
The SABPA study conforms to the principles outlined in
the Declaration of Helsinki (revised 2004) (World Medical
Association General Assembly 2004) and abided by the
institutional guidelines. It was approved by the ethics review
board of the North West University, South Africa (0003607S6).
All participants provided written informed consent.
The participants were in a semi-recumbent position for at
least 30 minutes prior to blood pressure (BP) measurements on
the non-dominant arm between 06:15 and 09:00 by a registered
nurse and doctor. They used a calibrated sphygmomanometer
(Riester CE 0124
®
) and a 1.3M
TM
Littman
®
II SE stethoscope
2205. Two duplicate measures were taken, with a three- to five-
minute resting period between each, the second of which was
used for statistical analyses.
Body height (stature), weight and waist circumference were
measured with calibrated instruments (Invicta Stadiometer, IP
1465, London, UK; Precision Health Scale, A&D Co, Tokyo,
Japan; Holtain unstretchable flexible 7-mm-wide metal tape,
Crosswell, Wales) while participants were in their underwear.
All measurements were done in triplicate by registered
anthropometrists according to standard procedures.
17
A registered nurse obtained fasting blood samples with a
sterile winged infusion set from the ante-brachial vein. EDTA
whole blood and serum were stored at –80°C. Venous samples
for fasting blood glucose were collected in sodium fluoride
tubes. All analyses were performed on samples drawn after an
overnight fast.
Plasma and serum samples were analysed using two sequential
multiple analysers (Konelab 20i; Thermo Scientific, Vantaa,
Finland; Unicel DXC 800, Beckman and Coulter
®
, Germany),
doing enzyme-linked immunosorbent assays (Quantikine enzyme-
linked immunosorbent assay, R&D Systems, Minneapolis, MN,
USA) for serum total and high-density lipoprotein (HDL)
cholesterol, serum triglyceride (TG), whole blood glycated
haemoglobin (HbA
1c
), fasting plasma glucose (FPG) and serum
insulin levels. The intra- and inter-coefficients of variation for all
assays were below 10%.
NT-proBNP serum samples were obtained at both baseline
and follow-up examinations and frozen at –80°C until analysis
in one batch in 2015 (ECLIA method; Roche Diagnostics, Basel,
Swittzerland) using Cobas e411 automated platform (inter-batch
variability: 4.6%; intra-batch variability: 4.2%).
Prevalent impaired glucose tolerance (IGT) at the baseline
examination was defined as FPG > 5.6 mmol/l or HbA
1c
> 5.7%.
The metabolic syndrome (MetS) was defined as any three of
the following markers exceeding cut-off points: central obesity
(waist ≥ 102 cm in men, ≥ 88 cm in women); raised triglycerides
[> 150 mg/dl (1.7 mmol/l) or specific treatment for this lipid
abnormality]; reduced HDL cholesterol level [< 40 mg/dl (1.03
mmol/l) in men, < 50 mg/dl (1.29 mmol/l) in women or specific
treatment for this lipid abnormality]; raised BP (systolic BP >
130 or diastolic BP > 85 mmHg, or treatment of previously
diagnosed hypertension); raised FPG [> 100 mg/dl (5.6 mmol/l),
or previously diagnosed type 2 diabetes mellitus].
Insulin resistance was defined as the upper quartile of
homeostatic model assessment of insulin resistance (HOMA-
IR), which was calculated according to: (glucose × insulin)/22.5.
Prevalent and incident diabetes were defined as clinical diagnosis
of diabetes and/or use of anti-diabetic medication. History of
kidney disease and cardiovascular disease (defined as diseases
affecting the heart or blood vessels) were assessed through
questionnaires. Hypertension was defined as systolic BP > 140
mmHg or diastolic BP > 90 mmHg or use of antihypertensive
medication.
Overweight was defined according to ethnic cut-off points
18,19
as waist circumference (WC) ≥ 90 cm in African men, and ≥ 98
in African women, together with WC ≥ 94 cm in Caucasian men,
and WC ≥ 80 cm in Caucasian women.
Statistical analysis
Variables that were skewed (NT-proBNP, TG and FPG) were
log-transformed before analysis. Groups were compared using
one-way ANOVA tests. We used linear regression analysis
adjusted for age and gender to examine the associations per one
standard deviation (SD) increment of log-transformed values of
NT-proBNP at baseline with weight, body mass index (BMI),
waist circumference, HbA
1c
, FPG, insulin, HOMA-IR and TG
values at baseline and re-examination. In order to get a true
perspective of the effect of changes of NT-proBNP in the linear
and logistic regression analysis, outcomes were related to one
standard deviation of change of the ln-transformed values of
NT-proBNP.
Logistic regression models were used to calculate: (1) odds
ratios (OR) for prevalent overweight, IGT, hypertriglyceridaemia,
the MetS and insulin resistance at baseline examination adjusted
for age and gender, and (2) OR for incident diabetes [patients
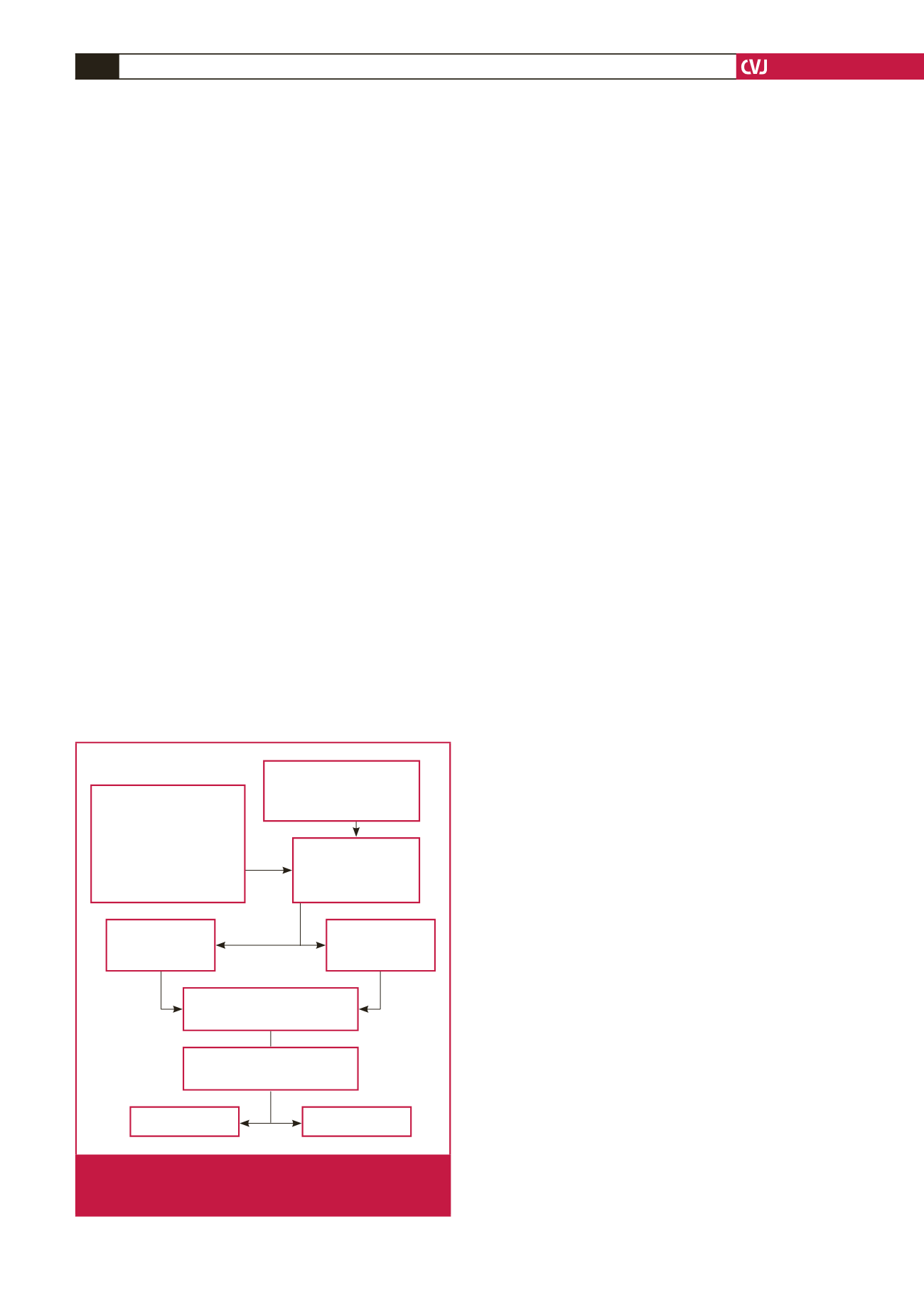
Exclusion criteria:
• Users of
α
- and
β
-blockers
• Psychotropic substance
abuse
• Blood donors/vaccinated
in previous 3 months
• Tympanum temperature
> 37.5°C
African and Caucasian
bi-ethnic gender cohort, aged
20–65 yrs invited:
n
= 2 170
screen:
n
= 471
Phase 1:
Non-responders: 62
Responders: 409
eligible and enrolled
Phase 2:
3-year follow up (359)
Exluding:
Missing NT-proBNP values (12)
Caucasian (209)
101
108
Africans (200)
101
99
Caucasian (
n
= 203)
Africans (
n
= 194)
Fig. 1.
Designof thebi-ethnic gender cohort of theSympathetic
activity and Ambulatory Blood Pressure in Africans
prospective study.