


















 37 / 64
37 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 6, November/December 2020
AFRICA
317
of AO and the MetS, with larger differences observed in men
compared to women.
The resulting over- or underestimation of AO, leading to the
same for the MetS, may have a negative impact on preventative
measures or interventions developed. For instance, with
overestimation of the prevalence of the MetS, individuals who
are at a relatively low risk would be incorrectly identified and
targeted for interventions. This in turn might lead to expenditure
directed at a cause that is unnecessary, which would be of
particular concern to health resource-poor countries such as
Botswana. Likewise, if the MetS is underestimated, individuals
at a high risk of developing cardiovascular diseases or diabetes
would be misdiagnosed or not identified and not targeted by
preventative measures aimed at a high-risk population.
It is therefore imperative that population-specific AO
cut-off values are determined from large, representative studies,
validated and used to determine population-specific risk factors.
Further analysis of the results according to gender is necessary
as vital information might be overlooked when only considering
the sample as a whole. The results from such studies will allow
for a more accurate estimation of the ever-changing prevalence
levels of the MetS over time, and in response, appropriate and
culturally sensitive interventions can be developed.
Evidence from several studies in which the optimal cut-off
values for AO were reported in SSA populations showed an
emerging trend (Table 3). From the comparisons, the trend is
higher WC cut-off values for the men than the women. The WC
cut-off points for women seem to be approximately 82 cm, which
is similar to the IDF recommendation.
9
It can then be argued that
irrespective of the optimal cut-off points for SSA populations,
WC for men appears to be higher than for women, and that for
women, values are most probably similar to IDF criteria.
This study presented several limitations. Cluster randomisation
is the recommended sampling method since the results would be
more inferable to the general population. However, targeting
malls excluded a portion of the population that does not
frequently visit malls, making it impossible to generalise to the
population as a whole. The study included only an urban-based
population, but only 69.4% of the Botswana population is
urbanised according to the 2018 revised United Nations world
urbanisation prospects.
20
The relationship between AO and
the MetS may be modulated by urbanisation and confounding
factors such as dietary habits, physical activity patterns as well
as general health.
21
It would be interesting to conduct a similar study in a rural
or peri-urban area and compare the findings to this study.
Furthermore, it would be recommended to include additional
data collection on diet, physical activity, food security and
general health. It is well known that Botswana is burdened with
a high HIV prevalence and that this could also influence the
prevalence of the MetS in this population.
Conclusion
The results of several studies have indicated that WC cut-off
values for AO are ethnic and gender specific.
8,11,18
It is highly
probable that the values may be even more variable among
different SSA populations. It is therefore imperative to investigate
whether this is indeed the case to aid in lowering the burden of
the MetS on the public health sectors. It is possible to establish
population- and gender-specific cut-off values for different
ethnic groups that can be used to classify AO in these ethnic
groups. Correctly identifying the MetS will go along way in
decreasing disease risk factors.
This work was supported by a grant from the office of Research and
Development of the University of Botswana round 24 (ref. no. UBR/RES
3/2) and the Stellenbosch University’s African Collaboration grant DRTAN
(ACG). Opinions, findings and conclusions or recommendations expressed in
Table 2. Comparison of the IDF definition criteria with the
newly determined optimal cut-off values in determining
the prevalence of AO and the MetS
Variables
IDF values (≥ 94 cm men
≥ 80 cm women)
New values (≥ 91 cm men
≥ 8 2cm women)
AO (%)
All
47.9
47.4
Men
24.5
30.3
Women
69.6
63.3
MetS (%)
All
32.6
33.3
Men
19.9
24.5
Women
44.5
41.5
AO, obdominal obesity; MetS, metabolic syndrome.
Table 3. Comparison of this study’s determined
WC cut-off points with similar studies
Studies
Ethnicity
Men
(cm)
Women
(cm)
IDF criterion
Europeans
94
80
Current study
Batswana
91
82
Onen
et al
.
15
Batswana
98
85
Motala
et al
.
18
South African (Zulus)
86
92
Hoebel
et al.
19
South African (urban blacks)
91
84
Magalhaes
et al
.
16
Angolans
88
81
Ekoru and
Murphy
17
SSA (Benin, Nigeria, Democratic
Republic of Congo, Uganda, Kenya,
Tanzania, South Africa and Seychelles)
81
81
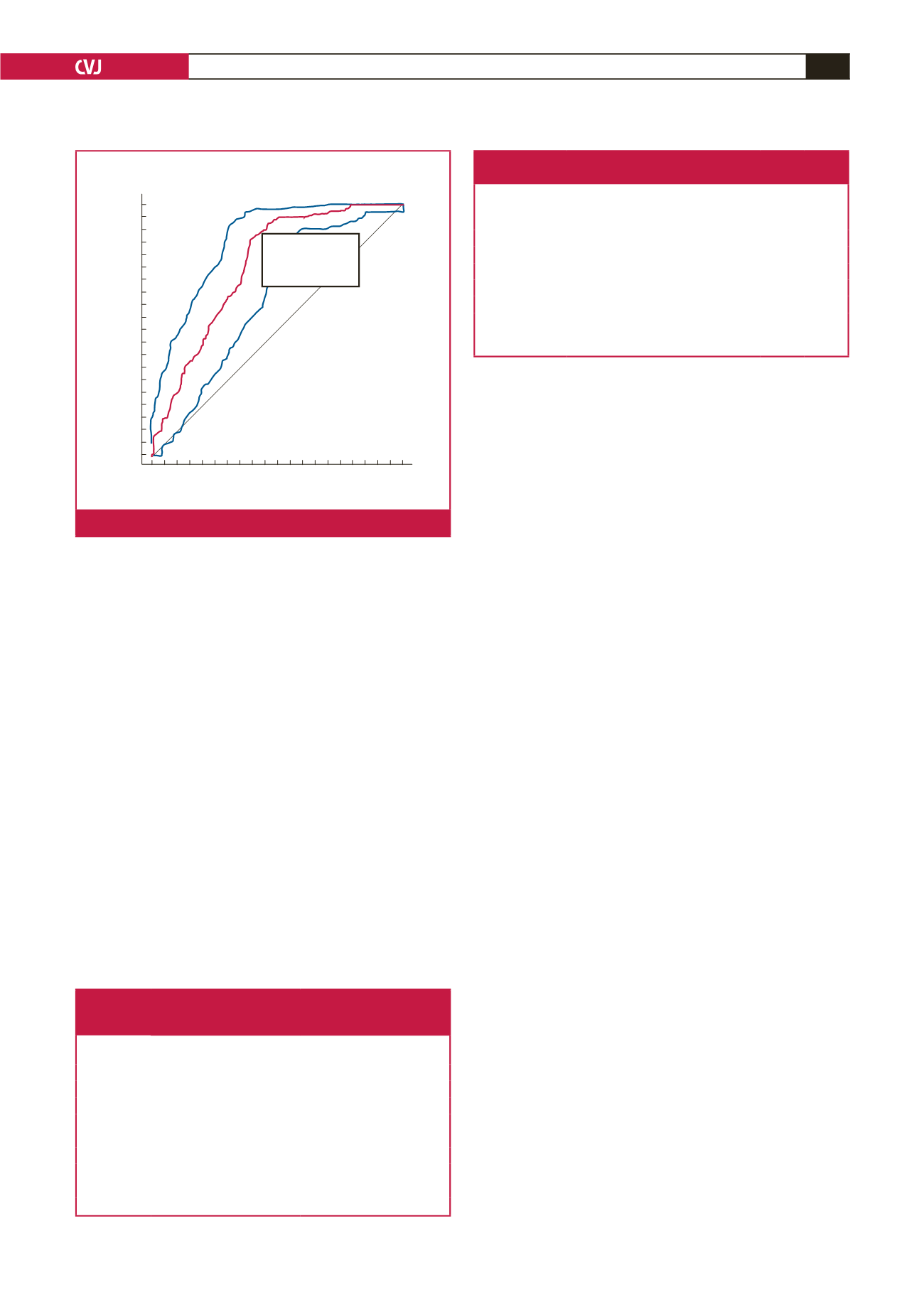
100-Specificity
100
80
60
40
20
0
0
20
40
60
80
100
Sensitivity
M9: Waist circumference
C1 = 0
Sensitivity: 88.6
Specificity: 58.9
Criterion: >82.3
Fig. 2.
ROC curve for the WC of females.