CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 3, May/June 2010
AFRICA
165
Discussion
PLSVC with absent RSVC (isolated PLSVC) is a very rare
venous malformation. During normal foetal development, the
left-sided anterior venous cardinal system regresses, leaving the
CS and the ligament of Marshall. Failure of the closure of the left
anterior cardinal vein results in PLSVC.
4
In general, PLSVC is
associated with RSVC and drains into the RA via a dilated CS.
When developmental arrest occurs at an earlier stage, the CS
is absent and the PLSVC drains into the LA. Either isolated or
associated with RSVC, this venous malformation itself causes
no haemodynamic disturbance and is usually diagnosed inci-
dentally.
5-7
However, it has several clinical implications. A PLSVC can
cause problems during central venous catheterisation (access to
the CS can cause hypotension, angina, perforation of the heart,
tamponade and arrest),
8
pacemaker implantation (due to the
circuitous path taken by the electrode, it can be difficult to obtain
a stable electrode position and sustained capture),
9
or cardiopul-
monary bypass (isolated PLSVC impairs the use of retrograde
cardioplegia).
In addition, a higher incidence of arrhythmias and conduc-
tion system abnormalities has been described in patients with
PLSVC. There are two proposed mechanisms for this asso-
ciation: a dilated CS stretches the atrioventricular nodal tissue,
which prepares a substrate for re-entrant tachycardias; or, the
early conduction tissue has close proximity to the cardinal
venous tissue and this leads to sinus node dysfunction. Lenox
et al
. found sino-atrial node abnormalities in some patients with
absent RSVC and this condition may predispose to sick sinus
syndrome.
10-12
In 10% of patients, a PLSVC may drain into the LA either
directly or via an unroofed CS. This creates a right-to-left shunt
and the risk of paradoxical embolism is markedly increased. In
addition, drugs directly enter the systemic circulation when they
are applied from the left brachiocephalic vein.
A final clinical implication of PLSVC (especially when
isolated) is a high incidence of accompanying congenital heart
defects, for example ventricular septal defect, atrial septal defect,
endocardial cushion defect or tetralogy of Fallot.
3,13
Therefore
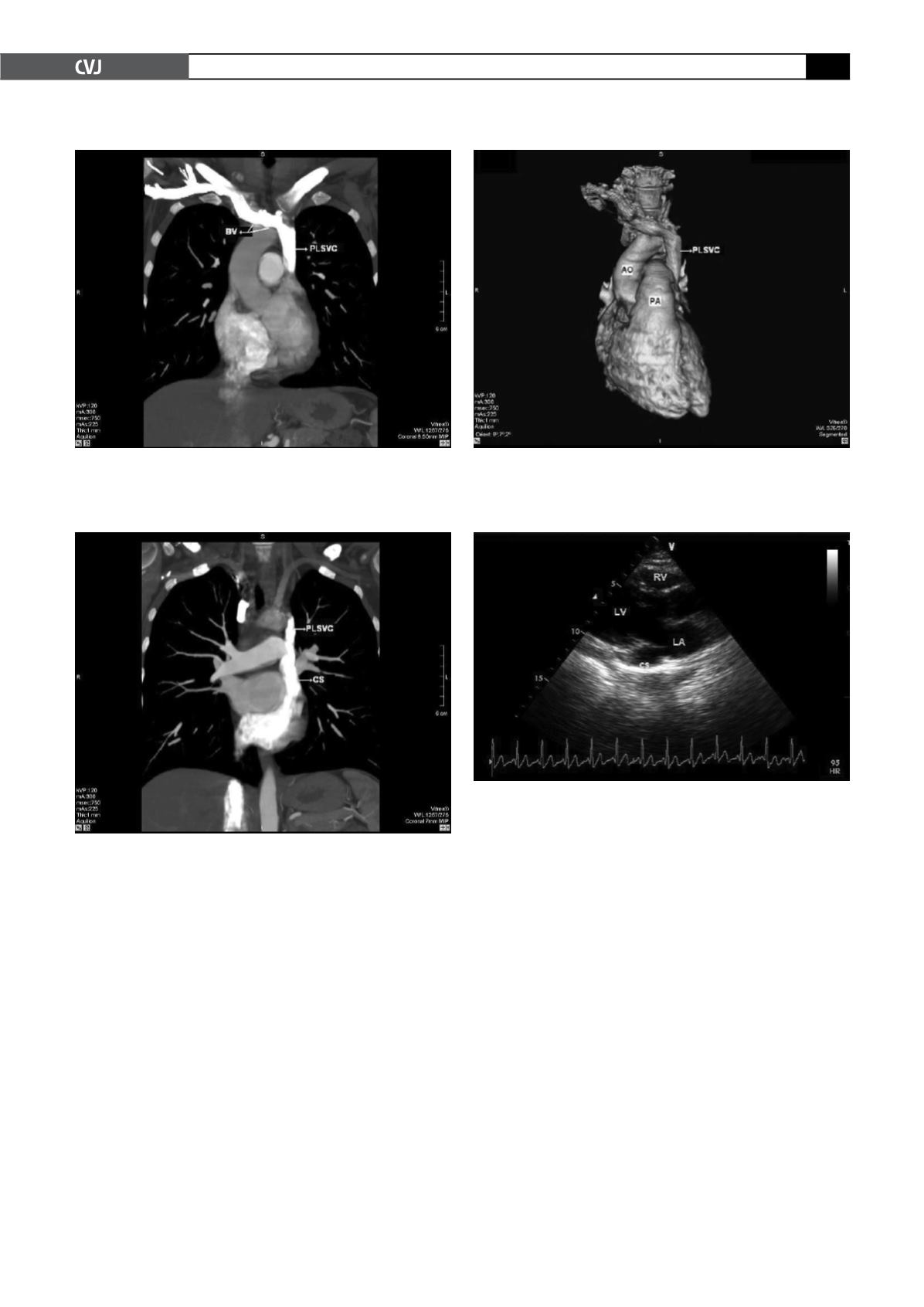
Fig. 4. Dilated coronary sinus (CS) on transthoracic
echocardiography, parasternal long-axis view (LA: left
atrium, LV: left ventricle, RV: right ventricle).
Fig. 2. Multiplanar reformatted image reveals the persist-
ent left superior vena cava (PLSVC) draining into a
dilated coronary sinus (CS).
Fig. 3. Volume-rendered, three-dimensional reconstruc-
tion of contrast-enhanced multi-detector computed tomo-
graphic image shows the persistent left superior vena
cava (PLSVC) descending on the left side of the thorax
(AO: aorta, PA: pulmonary artery).
Fig. 1. Multiplanar reformatted image demonstrates that
the right superior vena cava is absent and a bridging vein
(BV) drains the right jugular and subclavian veins, which
then join with the left brachiocephalic vein to form the
persistent left superior vena cava (PLSVC).


