CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 3, May/June 2011
146
AFRICA
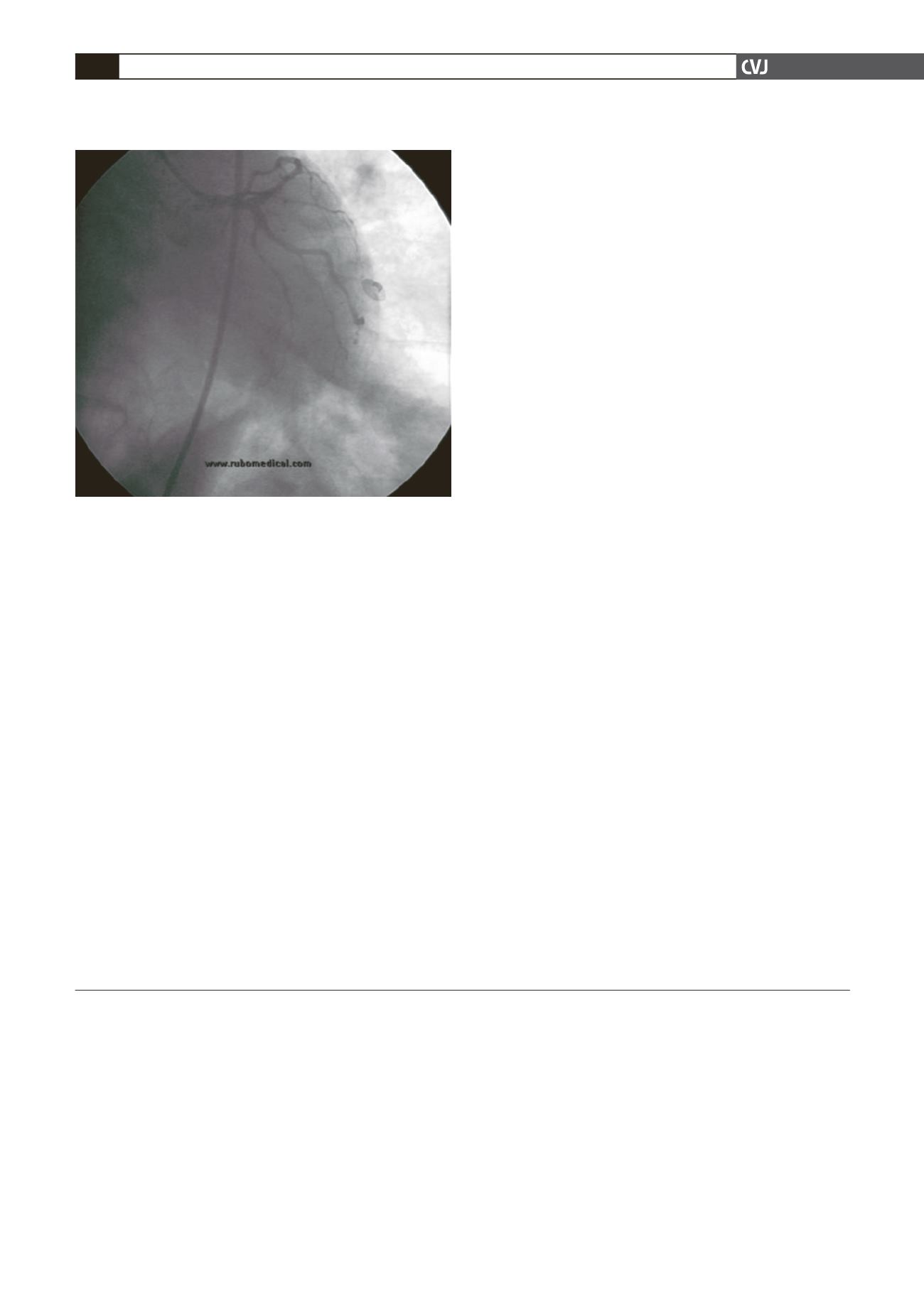
Minneapolis, USA). The stenting of the LMCA was done with
3.5
×
15-mm double-helix closed-cell Flex Force
®
stent (Aachen
Resonance, Germany) with good results. TIMI 3 flow was
achieved (Fig. 3).
After stenting the LMCA, we decided to stent the RCA. This
was done with a 2.75
×
12-mm Flex Force
®
stent. After restor-
ing the blood flow, the patient’s clinical status improved. He was
weaned off IABP and mechanical ventilation on day 2. He was
discharged from hospital on the seventh day in a stable condition.
After six months he was still asymptomatic.
Discussion
In this case we decided to perform LMCA and RCA stenting. In
the current guidelines, stenting for unprotected LMCA disease
is relatively more favourable in patients with isolated LMCA
lesions or LMCA plus single-vessel disease, for patients with
ostial or mid-LMCA lesions, and for those with co-morbidities
that would make CABG high risk or unlikely to be successful.
This is a class 2b recommendation.
3
Angiographic follow up
should not be done after six months or earlier, unless clinically
indicated by symptoms or myocardial ischaemia.
3
We believe full revascularisation must be done during cardio-
genic shock. In selected cases, with remote ischaemia, non-
infarct-related critical artery stenosis, and lack of haemodynamic
improvement after infarct-related artery percutaneous coronary
intervention (with IABP support), revascularisation of the non-
infarct territory may play a role.
4
A recent report suggests an
additive benefit of stenting plus glycoprotein IIb/IIIa antagonists
in cardiogenic shock, similar to the rest of the clinical spectrum
of percutaneous coronary intervention.
5
In conclusion, in a serious clinical condition such as cardio-
genic shock, stenting of the LMCA and non-infarct-related criti-
cal artery stenosis with intra-aortic balloon pump support must
be considered.
References
1.
Grygier M, Araszkiewicz A, Lesiak M,
et al
. Acute myocardial infarc-
tion in an 80-year-old woman caused by left main occlusion with
concomitant chronic total occlusions of right and left coronary artery:
successful treatment with percutaneous revascularization.
Cardiol J
2009;
16
: 568–572.
2.
McArdle H, Bhandari M, Kovac J. Emergency coronary stenting of
unprotected critical left main coronary artery stenosis in acute myocar-
dial infarction and cardiogenic shock.
Heart
2003;
89
: e24.
3.
Kushner FG, Hand M, Smith SC Jr,
et al
. 2009 focused updates: ACC/
AHA guidelines for the management of patients with ST-elevation
myocardial infarction (updating the 2004 guideline and 2007 focused
update) and ACC/AHA/SCAI guidelines on percutaneous coronary
intervention (updating the 2005 guideline and 2007 focused update)
a report of the American College of Cardiology Foundation/American
Heart Association Task Force on Practice Guidelines.
J Am Coll Cardiol
2009;
54
: 2205–2241.
4.
Menon V, Hochman JS. Management of cardiogenic shock complicat-
ing acute myocardial infarction.
Heart
2002;
88
: 531–537.
5.
Ajani AE, Maruff P, Warren R,
et al
. Impact of early percutaneous
coronary intervention on short- and long-term outcomes in patients
with cardiogenic shock after acute myocardial infarction.
Am J Cardiol
2001;
87
: 633–635.
Fig. 3. After successful percutaneous coronary interven-
tion.


