CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 2, March/April 2014
54
AFRICA
morphology of the underlying valve tissue was normal.
Eighteen (23.4%) patients (14 HIV uninfected and four
HIV infected) died during the course of the study (
p
=
ns).
Three HIV-uninfected patients died after surgery. One had
an aortic root abscess with fistula formation with coronary
ostial occlusion and died in theatre. The second died on day
seven in cardiogenic shock, and the third on day eight from an
intracerebral haemorrhage.
The CD
4
counts in the HIV-infected patients who died were
139, 135, 149 and 249/mm³. One of these patients underwent
emergency surgery for a disrupted right coronary cusp and died
35 days after surgery from a methicillin-resistant staphylococcal
(MRSA) septicaemia acquired postoperatively. The remaining
five HIV-infected patients who had surgery have not shown any
features of re-infection, and remained stable after one year.
Six patients (7.8%), all HIV negative, had advanced renal
involvement. Four were receiving haemodialysis at the time of
diagnosis.
Discussion
Few data exist on the clinical profile and echocardiographic
findings of IE in HIV-infected patients in the developing world.
8,9
Most reports of IE in HIV-infected individuals have focused
almost exclusively on IE in intravenous drug users, and it has
reportedly been rare in non-drug users.
10
In this study we have
shown that the clinical profile of IE in the HIV-positive patient
is similar to that in the HIV-negative patient, and is characterised
by fever, clubbing, murmurs and severe valve regurgitation.
In contrast to Western series,
10
the most common underlying
predisposing abnormality observed in our study was rheumatic
heart disease.
Vegetations occurred on the mitral and aortic valves and
there were three cases of right-sided endocarditis in patients
with congenital heart disease (two of whom were HIV infected.
The mean size of the vegetations was similar in both groups (11
mm) (Table 6); three out of the four patients with CD
4
counts
<
200/mm³ had slightly larger-sized vegetations (13 mm). These
findings are in keeping with the report by Smith
et al.
who
documented an 11.5% prevalence of infective endocarditis in
HIV-positive subjects with bacteraemia.
11
These authors showed
that there was no difference in the clinical characteristics of
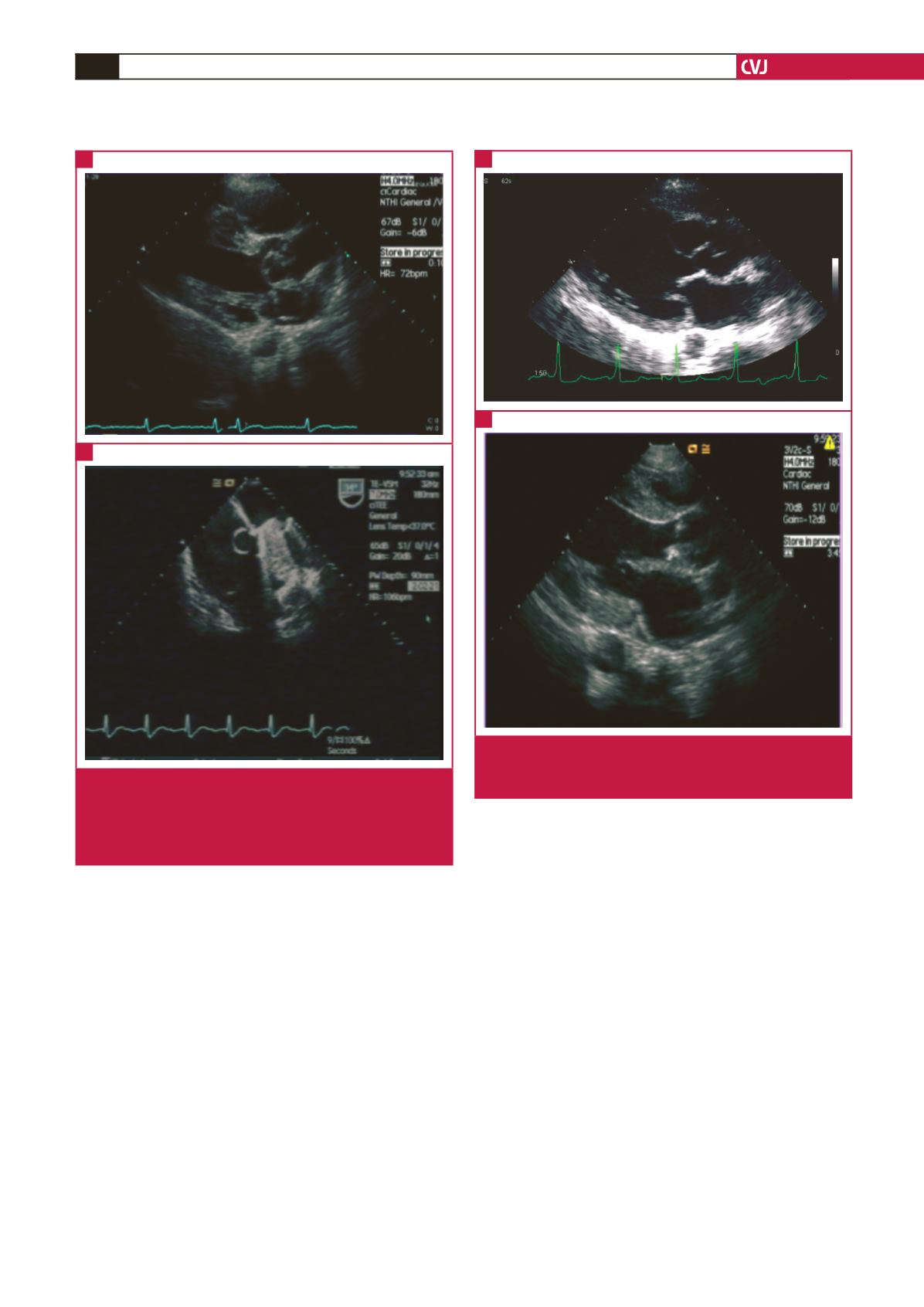
Fig. 2.
Leaflet aneurysm on the aortic and mitral valves in
an HIV-infected patient (parasternal long-axis view)
(A), and on the mitral annulus (arrows) (B), in the
HIV-negative patient with a mitral prosthesis (four-
chamber view on TEE).
A
B
Fig. 3.
Aortic root abscess involving the non-coronary cusp
(arrows) of the aortic valve in an HIV-infected (A), and
an HIV-negative subject (B).
A
B


