CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 2, March/April 2014
AFRICA
55
HIV-positive patients with and without IE.
11
We noted that leaflet aneurysms and aortic root abscesses
occurred in both HIV-positive and HIV-negative subjects, but
the numbers were too small for a formal statistical comparison.
In these cases, echocardiography revealed severe valve damage,
with peri-valvular extension of the infection leading to abscess
formation and/or the development of fistula, features associated
with a poor prognosis.
12
Three patients died in the immediate
postoperative phase (the first, coronary ostial occlusion, the
second had cardiogenic shock, and the third patient was HIV
positive and died from MRSA infection).
A relationship between aneurysms and the HIV infection
has been documented in vascular series,
13
in which aneurysms
have been found to be multiple and occur in unusual anatomical
locations. In our cases, the root abscesses and leaflet aneurysms
were larger in size in the HIV-positive patients. None of our
patients had evidence of mycotic aneurysms elsewhere, which
has been reported more frequently when presentation is delayed,
especially in developing countries.
14
In this study, pericardial effusion was a common finding
in both groups, and was attributed largely to severe valve
regurgitation and resulting heart failure. More than half (62%)
the patients with pericardial effusion had failure of leaflet
or cuspal coaption with a marked degree of haemodynamic
compromise. However, markedly impaired systolic function with
heart failure was not more frequent in HIV-negative patients.
Pericardial effusions are considered to be a common form
of cardiovascular involvement in HIV-infected individuals, the
cause of which includes tuberculosis and pyogenic infection,
particularly
S aureus
, as a result of endocarditis.
15
The six
patients with staphylococcal infection had small effusions that
were not aspirated. Four patients in each group had evidence
of extracardiac tuberculosis, but the cause of the pericardial
effusion in these patients was thought to be valve destruction
with heart failure.
In this study,
S aureus
was the most common infecting
bacterium, followed by
S viridans
. In the Western Cape,
Koegelenberg
et al
.
16
found that
S
viridans
is still the most
common bacterium in their group of HIV-positive patients. In
Western series,
S aureus
is the commonest causative organism in
HIV-infected patients; it is reported largely in intravenous drug
users and has a predilection for the tricuspid valve. None of the
patients recruited in our study were intravenous (‘mainline’)
drug users. We did not find any multi-resistant organisms in the
HIV-infected group. In the one HIV-infected patient with MRSA,
S aureus
was acquired postoperatively.
In our study, 42 patients had negative blood cultures, an
occurrence that was likely due to the setting of our study, a
Table 6. Echocardiographic features predictive of surgery
Echo finding
HIV+
n
=
17(%)
HIV–
n
=
60 (%)
Total
Vegetations
Persistence after stroke
1 (5.9)
–
1
>
10 mm
4 (23.5)
13 (21.7)
17
Increase in size
–
1 (1.7)
1
Valve dysfunction
Perforated leaflets
1 (5.9)
1 (1.7)
2
Valve regurgitation
16 (94.1)
55 (91.7)
71
Impaired LV function
–
3 (5)
3
Not responding to antibiotics
–
1 (1.7)
1
Paravalvular extension
Rupture/fistulae
–
1 (1.7)
1
Abscess/aneurysm
7 (41.2)
4 (6.7)
11
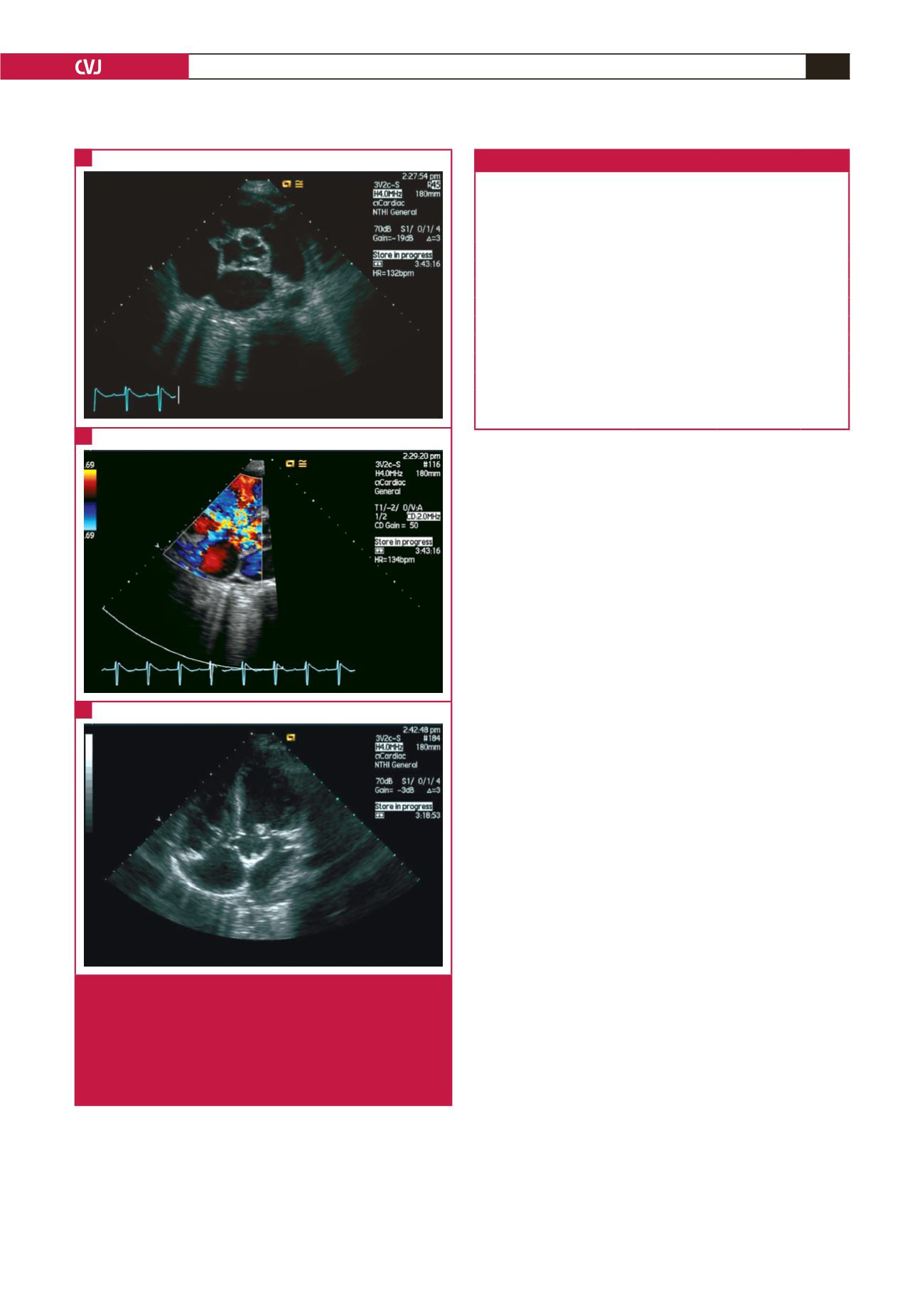
Fig. 4.
Fistulous connection between a root abscess and the
right atrium (arrow) in the parasternal short-axis view
of an HIV-negative patient (A). The colour Doppler
picture (B) shows flow across the fistulous connection
into the right atrium. Fistulous connection between
root abscess and right atrium (arrow) in the paraster-
nal five-chamber view (C).
A
B
C


