


















 48 / 68
48 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 1, January/February 2015
46
AFRICA
Patients who had multiple risk factors and those who had
symptoms of coronary artery disease (angina, ischaemic changes
on electrocardiography, ischaemia on dipyridamole thallium
scintigraphy, or left ventricular wall-motion abnormalities
on stress echocardiography) were evaluated by means of
pre-operative coronary angiography.
Coronary angiography was performed on three patients in
group 1. Two of these patients were treated with angioplasty. In
group 2, coronary angiography was performed on four patients
and one required angioplasty. None of the patients required
surgical intervention for coronary artery disease.
Mean follow-up time was 46.5
±
27.7 (5–125) months in group
1 and 48.6
±
29.6 (6–117) months in group 2. All operations were
performed under general anaesthesia.
Surgical procedure in the conventional method
The femoral arteries were explored under the inguinal ligament
and appropriate anastomosis sites were examined. The abdomen
was explored with upper and lower median incisions. The
abdominal aorta was explored and after deciding on the
appropriate anastomosis site, the aorta was suspended with
nylon tape.
Before heparinisation, transperitoneal tunnels were created
between the femoral areas and the anastomosis site using a
long, blunt-tipped forceps. A long nylon tape was transferred
through the tunnel and left inside. After tunnelling, the patient
was heparinised and the aortic anastomosis was performed.
The nylon tape was then left and the previously created tunnel
walls were stretched. Forceps were introduced a second time
from the femoral area to the anastomosis site. The distal end
of the graft was clasped and pulled through to the femoral
area (Fig. 1). The same procedure was applied on the other
side. Femoral anastomosis was performed and a drain was left
intraperitoneally before closure.
Surgical procedure with nylon tape
The same procedure as in the conventional methodwas performed
up to the aortic anastomosis. The distal ends of the graft were
tied to the nylon tape and the aortic clamp was opened. The graft
filled with blood. The femoral end of the nylon tape was pulled
and the graft was introduced into the femoral area. The same
procedure was applied for the other side (Figs 2, 3). Thereafter,
the operation was continued as in the conventional method.
Results
The mean age was 60.98
±
11.92 (37–92) years in group 1 and
62.88
±
9.22 (43–81) years in group 2. There was no significant
difference between the groups in terms of co-morbidity factors
such as diabetes mellitus, coronary artery disease, chronic
obstructive pulmonary disease and hyperlipidaemia (
p
>
0.05).
Hypertension was significantly higher in group 2 patients (
p
<
0.05). Pre-operative data of both groups are summarised in
Table 1.
When we compared operative data, we found that operation
length was 246
±
101.62 minutes in group 1 and 231.38
±
65
minutes in group 2. Despite the operation length being shorter
in group 2, it was not statistically significantly different (
p
>
0.05). There was no significant difference between the groups for
additional vascular procedures. Operative data of the groups are
summarised in Table 2.
When we compared postoperative data, there was no
significant difference between the groups in terms of extubation
time, intensive care length of stay, revision for bleeding, other
postoperative complications [such as sexual dysfunction, nerve
damage, secondary aorto-enteric fistula (SAEF), ileus, vascular
injury or acute renal failure], infection and rehospitalisation
for late-term infection (
p
>
0.05). Hospital length of stay and
blood usage were significantly higher in group 1 (
p
<
0.05).
Postoperative drainage levels were higher in group 1, but not
statistically significantly different (
p
>
0.05) (Table 3). Mortality
rates were similar in the two groups (
p
>
0.05).
In group 1, three patients died, two because of multiple organ
failure and one because of myocardial infarction at late term. In
group 2, two patients died, both because of multiple organ failure.
Fig. 1.
The graft tied to the nylon tape.
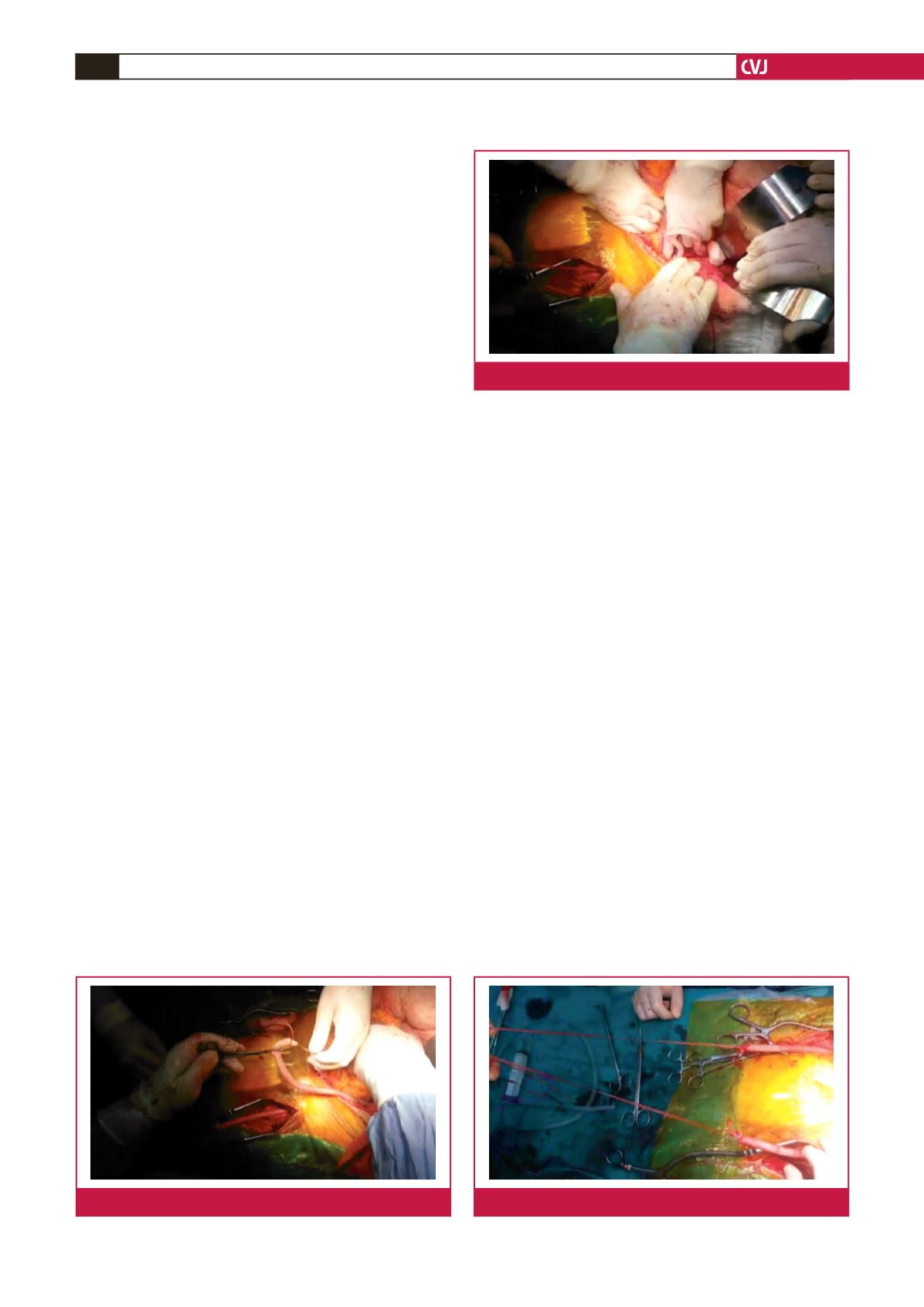
Fig. 2.
The graft being pulled through with the nylon tape.
Fig. 3.
After transferal of the graft using the nylon tape.