


















 52 / 68
52 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 1, January/February 2015
e2
AFRICA
In the late follow after five years, she was in NYHA class
I. TEE revealed reduced interventricular septum thickness (12
mm), normal left ventricular function with a mean 10 mmHg
and peak 20 mmHg gradients across the mechanical aortic valve.
The peak gradient on the mechanical mitral valve was 6 mmHg.
The right ventricle was normal with no regurgitation on the
pulmonary valve.
Discussion
Aortoventriculoplasty, known as the Konno procedure, was
first performed in October 1974 and was reported in 1975.
1
AVP
is an established method of reconstruction of complex LVOT
obstruction by the insertion of an adequately sized mechanical
valve prosthesis after patch enlargement of the aortic annulus
and septum. This method allows the implantation of a prosthetic
valve, three or four sizes larger than the original size of the
annulus.
It seems to be the most acceptable procedure in a patient with
LVOT obstruction and concomitant MVR, since a mechanical
mitral valve excludes the possibility of posterior annuloplasties
such as the Nicks and Manouguian procedures.
5
We chose
to perform aortoventriculoplasty because our patient had
previously undergone AVR and MVR and echocardiography
showed increased interventricular septum thickness with small
aortic root.
Left ventricular function after AVP is important because the
Konno procedure involves a longitudinal aortoseptal incision
through a right ventricle incision.
6
The incision must be made
parallel to the pulmonary artery ring. This incision could lead
to maintenance of the left ventricular function and prevent
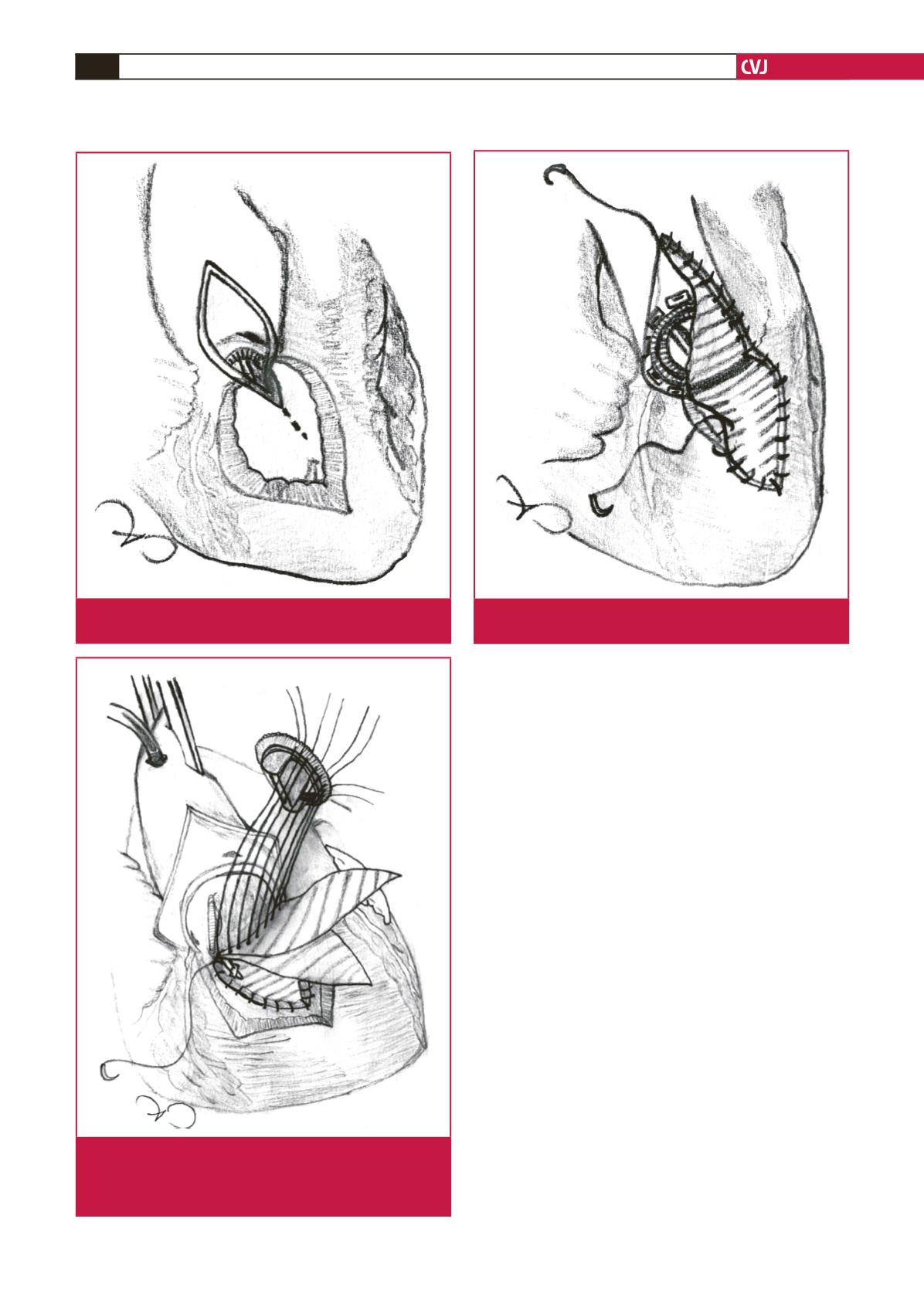
Fig. 2.
The left ventricular outflow tract is reconstructed with
two diamond-shaped patches. A no 23 St Jude pros-
thetic valve was implanted with interrupted stitches
with Teflon felt.
Fig. 3.
The aorta and right ventricular outflow tract recon-
structed with the patches.
Fig. 1.
Vertical aortatomy, incision in the right ventricular
outflow tract and the ventricular septum.