
















 40 / 67
40 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 2, March/April 2015
86
AFRICA
Spontaneous coronary artery dissection associated with
fibromuscular dysplasia
Anthony J Dalby, Lewis J Levien
Abstract
This case presentation concerns a woman known to have
fibromuscular dysplasia (FMD) who presented with an acute
coronary syndrome (ACS). The coronary angiogram was
considered to be normal. However, as spontaneous coronary
artery dissection (SCAD) has a close association with FMD,
subsequent meticulous review of the angiogram revealed
a dissection within the circumflex coronary artery. SCAD
causes 10% of ACS seen in women under 55 years of age.
Both FMD and SCAD are underdiagnosed and SCAD may
be overlooked or misdiagnosed on coronary angiography. The
recommended management of SCAD differs from that of the
usual presentations of ACS. For this reason, one should be
alert to the possibility of SCAD when confronted by ACS in a
younger woman, especially when she is known to have FMD.
Keywords:
acute coronary syndromes, fibromuscular dysplasia,
spontaneous coronary artery dissection
Submitted 30/10/14, accepted 22/1/15
Cardiovasc J Afr
2015;
26
: 86–90
www.cvja.co.zaDOI: 10.5830/CVJA-2015-009
The average age of women presenting with acute coronary
syndrome is 72.7
+
11.3 years.
1
Acute myocardial infarction,
an unusual occurrence in younger women, is more frequently
associated with non-atherosclerotic conditions than the infarcts
encountered in men or older women. A large number of
non-atherosclerotic causes of myocardial infarction have been
recognised. This case report concerns an acute myocardial
infarction caused by spontaneous coronary artery dissection in a
woman known to have fibromuscular dysplasia (FMD).
Case report
The patient was a 51-year-old post-menopausal Caucasian
woman who had been diagnosed with mitral valve prolapse and
exercise-induced palpitations for which she was on treatment
with a beta-blocker. She was also on hormone replacement
therapy with a fixed combination of estradiol and drospirenone.
Four years earlier she had undergone bilateral iliac artery
angioplasties by one of us (LJL) for symptomatic FMD. At that
time her angiogram showed the typical changes of iliac FMD (Fig.
1) as well as FMD involving her renal arteries. In addition both
carotid arteries manifested ultrasound features, suggesting FMD.
Four months prior to this presentation she had been assessed
by a cardiologist (AJD) for bouts of left-sided chest pain
unrelated to exertion that would last two to three hours at a time
and were associated with nausea. She was a non-smoker with no
history of hypertension or diabetes. Her total serum cholesterol
was 5.4 mmol/l with a low-density lipoprotein cholesterol level
Milpark Hospital, Johannesburg, South Africa
Anthony J Dalby, FCP (SA), FACC, FESC,
ajd@hot.co.zaSunninghill Hospital, Johannesburg
Lewis J Levien, MB BCh, FCS (SA), PhD Med)
Case Reports
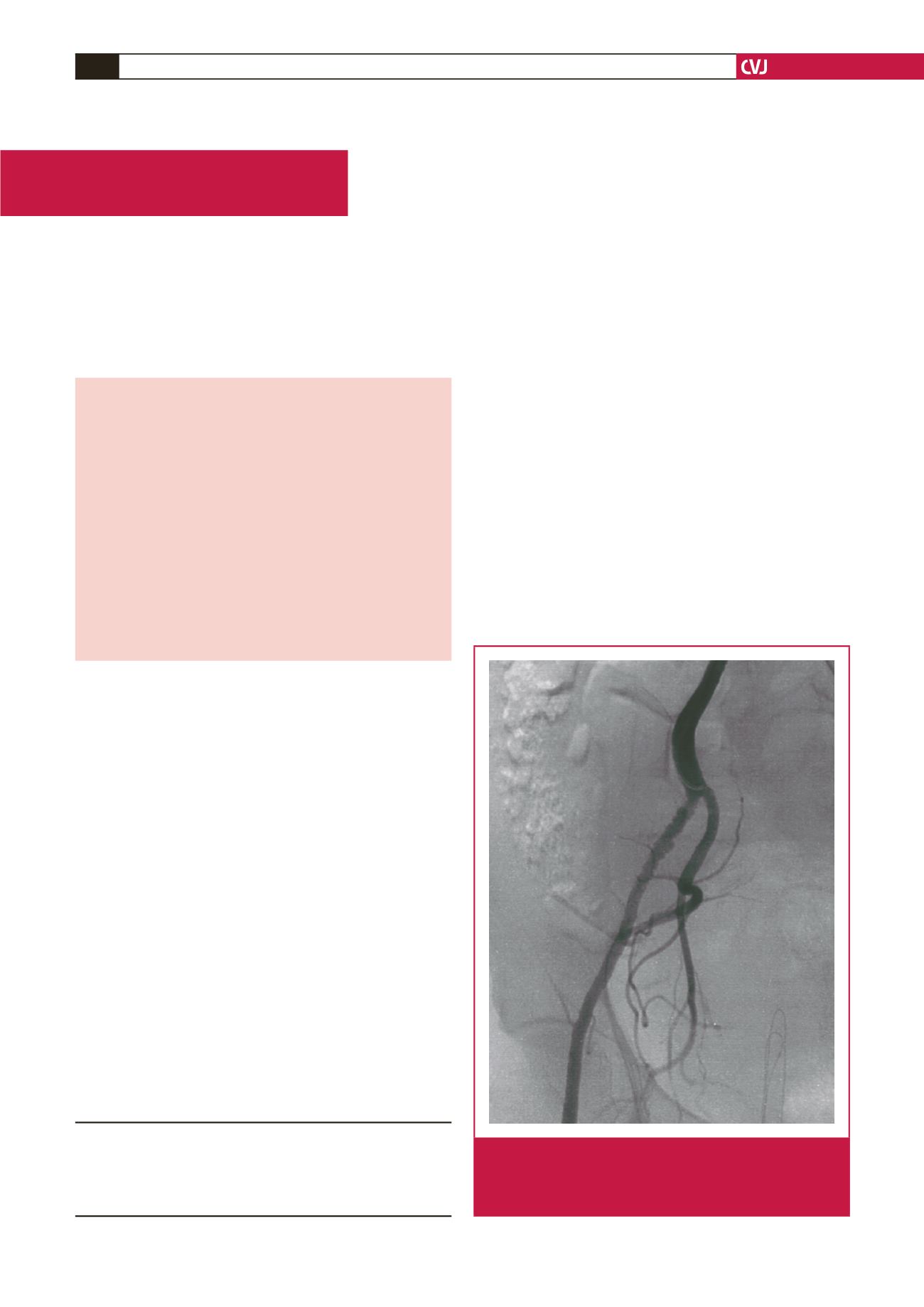
Fig. 1.
The patient’s iliac angiogram before angioplasty
showing the ‘string of beads’ deformity of the vessel
lumen with alternate stenosis and beading. Typically
the beads extend beyond the normal lumen diameter.