
















 42 / 67
42 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 2, March/April 2015
88
AFRICA
Discussion
Non-atherosclerotic coronary artery disease (NACAD) arises in
a number of diverse conditions (Table 1), of which not all are
associated with apparently normal appearances on the coronary
angiogram. In a series reviewing a large number of coronary
angiograms, it was noted that only 2.3% had been performed
in women under the age of 50 years; 42.9% of this subgroup
had presented with an acute coronary syndrome and 37.3% had
an elevated troponin level. While slightly more than half had
normal vessels, atherosclerotic disease was present in 30.5%, and
13.0% had NACAD.
2
FMD is a disease of uncertain aetiology.
3
It manifests as
a non-inflammatory, non-atherosclerotic fibrous proliferation
most commonly involving the arterial media (80–90%), although
it may affect the intima (10%) or adventitia/peri-arterial tissue
(
<
5%).
4,5
The condition is predominantly encountered in middle-
aged women (female-to-male ratio 9:1), although it may be
encountered in children and adolescents.
FMD appears to have a genetic basis as 7–11% of the first-
degree relatives of patients with FMD are similarly affected.
6
Hormonal influences or developmental ischaemia arising from
the vasa vasorum also have been considered as a possible cause.
3
The renal arteries are affected in 58–75% of cases, the carotid/
vertebral arteries in 32% and other arteries in 10%.
4
FMD has
been reported to be present in 2.6–4.4% of the renal arteries of
transplant donors.
7
FMD most commonly causes hypertension due to renal
artery stenosis, accounting for approximately 10% of all cases of
renovascular hypertension. The development of kidney failure
is rare.
4
FMD less frequently causes stroke due to carotid or
vertebral artery dissection, or claudication due to involvement
of the iliac arteries. Intracranial aneurysms have been observed.
The mesenteric, upper (particularly brachial) or lower limb
(iliac) arteries may be affected. Coronary involvement has been
regarded as uncommon.
FMD may present with any of a large variety of symptoms
depending upon the location and severity of the vascular
lesion/s. Hypertension, headache, pulsatile tinnitus, dizziness,
a cervical bruit and neck pain are the most frequent.
5
Because
FMD presents with non-specific symptoms, it is perceived as
a rare disease and is poorly understood by clinicians, which
often results in delays in diagnosis, frequently by several
years.
5
Table 1. Causes of non-atherosclerotic coronary
artery disease (NACAD)
Spontaneous coronary artery dissection (SCAD)
Fibromuscular dysplasia (FMD)
Ehlers-Danlos type IV
Marfan’s syndrome
Coronary FMD
Ectasia
Vasculitis
Systemic lupus erythematosis
Takayasu’s arteritis
Coronary spasm
Prinzmetal angina
Cocaine use
Embolism
Any source of cardio-embolism
Takotsubo or stress cardiomyopathy
Congenital anomaly
Myocardial bridging
Uncertain aetiology
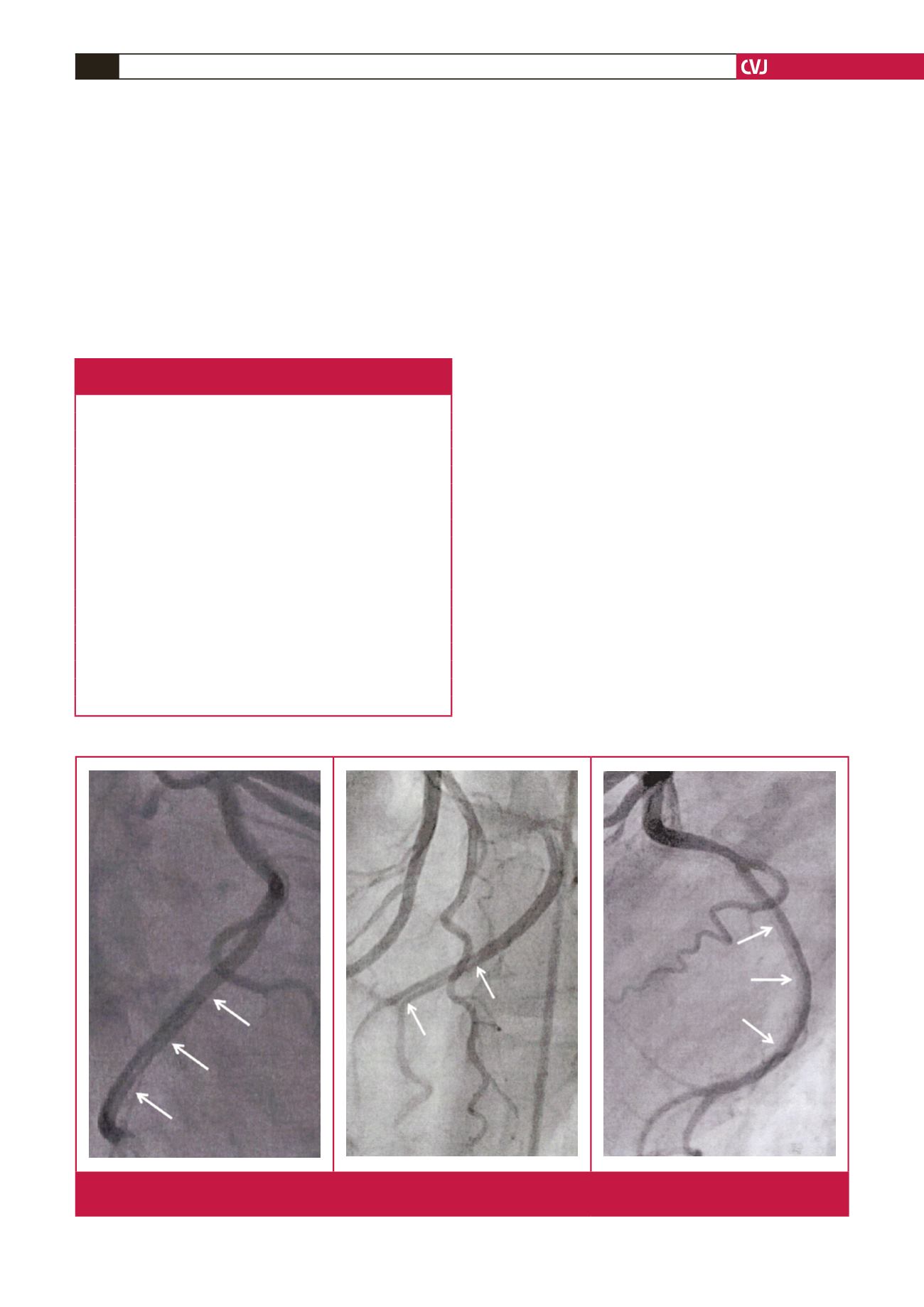
Fig. 4.
Magnified still-frame views (right anterior oblique, left anterior oblique and left lateral) from the patient’s initial angiogram
demonstrating the long dissection within the circumflex artery (arrows indicate the dissection).