
















 44 / 67
44 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 2, March/April 2015
90
AFRICA
References
1.
Perl L, Bental T, Assali A,
et al
. Impact of female sex on long-term acute
coronary syndrome outcomes.
Coron Artery Dis
2014; Epub ahead of
print. PMID: 25144669.
2.
Saw J, MD, Aymong E, Mancini GBJ,
et al
. Nonatherosclerotic coro-
nary artery disease in young women.
Can J Cardiol
2014;
30
; 814–819.
DOI:10.1016/j.cjca.2014.01.011.
3.
Stanley JC, Wakefield TW. Arterial fibrodysplasia. In: Rutherford R
(ed).
Vascular Surgery
. 6th edn. Phildelphia: Elsevier, 2005: 432–452.
4.
Chrysant SG, Chrysant GS. Treatment of hypertension in patients
with renal artery stenosis due to fibromuscular dysplasia of the renal
arteries.
Cardiovasc Diagn Ther
2014;
4
: 36–43. DOI:10.3978/j.issn.2223-
3652.2014.02.01.
5.
Olin JW, Gornik HL, Bacharach JM,
et al
. Fibromuscular dysplasia:
state of the science and critical unanswered questions. A scientific
statement from the American Heart Association.
Circulation
2014;
129
:
1048–1078. DOI:10.1161/01.cir.0000442577.96802.8c.
6.
Perdu J, Boutouyrie P, Bourgain C,
et al
. Inheritance of arterial lesions
in renal fibromuscular dysplasia.
J Hum Hypertens
2007;
21
; 393–400.
PMID: 17330059.
7.
Andreoni KA, Weeks SM, Gerber DA,
et al
. Incidence of donor
renal fibromuscular dysplasia: does it justify routine angiography?
Transplantation
2002;
73
; 1112–1116. PMID: 11965042.
8.
Savard S, Steichen O, Azarine A,
et al
. Association between 2 angio-
graphic subtypes of renal artery fibromuscular dysplasia and clini-
cal characteristics.
Circulation
2012;
126
: 3062–3069. DOI:10.1161/
CIRCULATIONAHA.112.117499.
9.
Michelis KC, MD, Olin JW, DO, Kadian-Dodov D,
et al
. Coronary
artery manifestations of fibromuscular dysplasia.
J Am Coll Cardiol
2014;
64
: 1033–1046. DOI: 10.1016/j.jacc.2014.07.014.
10. Lempereur M, Gin K, Saw J. Multivessel spontaneous coronary artery
dissection mimicking atherosclerosis.
J Am Coll Cardiol Intv
2014;
7
:
e87–88. DOI:10.1016/j.jcin.2013.12.207.
11. Cheema AN, Al Lawati H, Bagai A,
et al
. Spontaneous coronary artery
dissection in young women presenting with acute coronary syndrome:
angiographic findings from the GENESIS PRAXY Study.
J Am Coll
Cardiol
2014;
63
: A3 (Abstract).
12. Saw J, Ricci D, Starovoytov A et al. Spontaneous coronary artery dissec-
tion. Prevalence of predisposing conditions including fibromuscular
dysplasia in a tertiary center cohort.
J Am Coll Cardiol Intv
2013;
6
: 44
–52. DOI:10.1016/j.jcin.2012.08.017.
13. Prasad M, Liang J, Hayes S,
et al
. Extracoronary vascular abnormalities
are common in patients with spontaneous coronary artery dissection:
Analysis of 72 patients at a tertiary referral center.
J Am Coll Cardiol
2014;
63
, A2057 (Abstract).
14. Tweet MS, Hayes S, Gulati R,
et al
. The risk of pregnancy after spon-
taneous coronary artery dissection.
J Am Coll Cardiol
2014;
63
, A5
(Abstract).
15. Alfonso F, MD, Paulo M, Gonzalo N,
et al
. Diagnosis of spontaneous
coronary artery dissection by optical coherence tomography.
J Am Coll
Cardiol
2012;
59
: 1073. DOI:10.1016/j.jacc.2011.08.082.
16. Alfonso F, Bastante T, Rivero F,
et al
. Spontaneous coronary artery
dissection – from diagnosis to management.
Circ J
2014;
78
: 2099–2110.
DOI:10.1253
/circj.CJ-14-0773.
17. Tweet MS, Hayes SN, Pitta SR,
et al
. Clinical features, management, and
prognosis of spontaneous coronary artery dissection.
Circulation
2012;
126
: 579–588. DOI:10.1161/CIRCULATIONAHA.112.105718/-/DC1.
Erratum
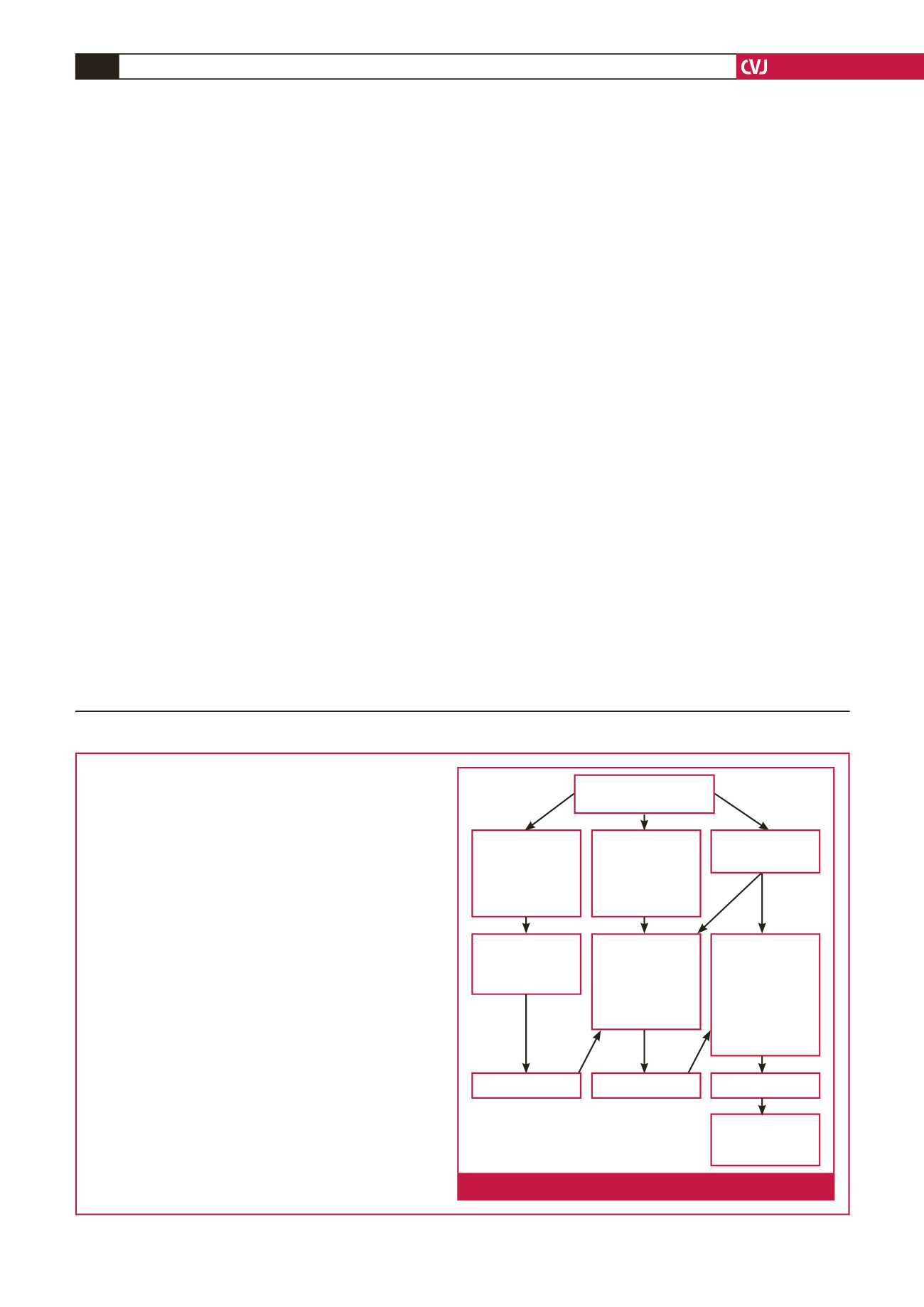
We regret the error in Figure 1 of the review article in
Cardiovasc J Afr
25
(6): 288
South African hypertension practice
guideline 2014
Hypertension guideline working group:
YK Seedat, BL Rayner, Yosuf Veriava
This is the correct figure.
Measure BP on at
least three occasions
BP 140–159/
90–99 mmHg
with < 3 risk
factors, no TOD
or complications
BP 140–159/
90–99 mmHg
with ≥ 3 risk
factor, diabetes,
TOD or
complications
Lifestyle
modification and
commence two
drugs preferably
in fixed-drug
combination,
review in 4–6
weeks
Lifestyle
modification
and commence
monotherapy,
review in 4–6
weeks
Lifestyle
modification for
3–6 months
Not at goal
Add third drug/
optimise doses of
drugs
*BP > 180/110 mmHg refer to section 9
BP ≥ 160/
100 mmHg*
Not at goal
Not at goal
Fig. 1.
Overview of approach to treatment.