
















 70 / 102
70 / 102

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 3, May/June 2016
192
AFRICA
the United States, which has one EP per 127 500 people, it is
estimated that South Africa needs a further 400 EPs for the
equivalent population!
The way forward
Having identified the profound deficiencies in the training
of cardiologists, cardiothoracic surgeons and paediatric
cardiologists in our country, the SA Heart Executive Committee,
at three National Council face-to-face meetings held in 2015,
identified the need to prepare a position paper summarising the
facts and exact training deficiencies in South Africa over the
past decade. It was generally felt that specialists in academia
and private practice need to work more closely together and
endeavour to engage with members of the Departments of
Health and Education. In addition, the pharmaceutical, device
and private hospital groups should be encouraged to sponsor
more training posts in academic institutions.
To facilitate earlier disease detection (e.g. RHD in young
adults, including pregnant women) in a country and continent
with so few specialists per capita, capacity for screening will
have to be increased. This could be achieved by training a larger
group of healthcare workers in the appropriate use of simple,
hand-held ultrasound devices. The screening for relevant diseases
requiring referral to secondary and tertiary facilities could then,
to some extent, be performed by general practitioners and
medical technologists.
24
In cases of women presenting with cardiac symptoms in
pregnancy, the obstetricians could receive training in screening
for cardiac diseases, as is currently already in practice via a
dedicated clinic at Groote Schuur Hospital. Obstetricians have
good ultrasound skills and the detection of turbulence over a
rheumatic valve, a myopathic heart or a pericardial effusion
would lead to quicker referral to cardiologists or cardiothoracic
surgery for appropriate intervention.
SA Heart is cognisant of the fact that the health authorities
face tremendous challenges. Mismanagement and a burgeoning
layer of bureaucracy have had a catastrophic effect on the delivery
of healthcare. This deficiency is evident at all levels, including the
training of nurses and specialists, and the provision of an adequate
infrastructure for the practice of an acceptable level of medicine.
Fundamental to this issue is the failure by the government to
recognise that academic and tertiary health facilities are not a
burden to the economy but underpin a strong and effective health
system. In particular, provincial government has abrogated its
responsibility to support and promote tertiary medicine, which
has culminated in poor service delivery to the indigent patient and
plummeting morale among the academic community.
In the setting of very limited resources and previously poorly
investigated sectors of the population, it is very important
that cardiologists are trained to deal with a broader range of
disorders so that they are recognised and appropriately managed
away from the few teaching hospitals. In such hospitals, it is
important to have good support for emerging subspecialities
within cardiology to integrate service, teaching and research
that is relevant to this country. Specific areas that need attention
include cardiology in pregnancy, heritable disorders predisposing
to cardiomyopathy and arrhythmia, and metabolic disorders
including especially familial hypercholesterolaemia, in which
much progress in treatment has been made. Rumours that
management of tertiary hospitals will be taken over by the
national government seem promising but unlikely to occur any
time soon.
The committee has summarised gaps and possible
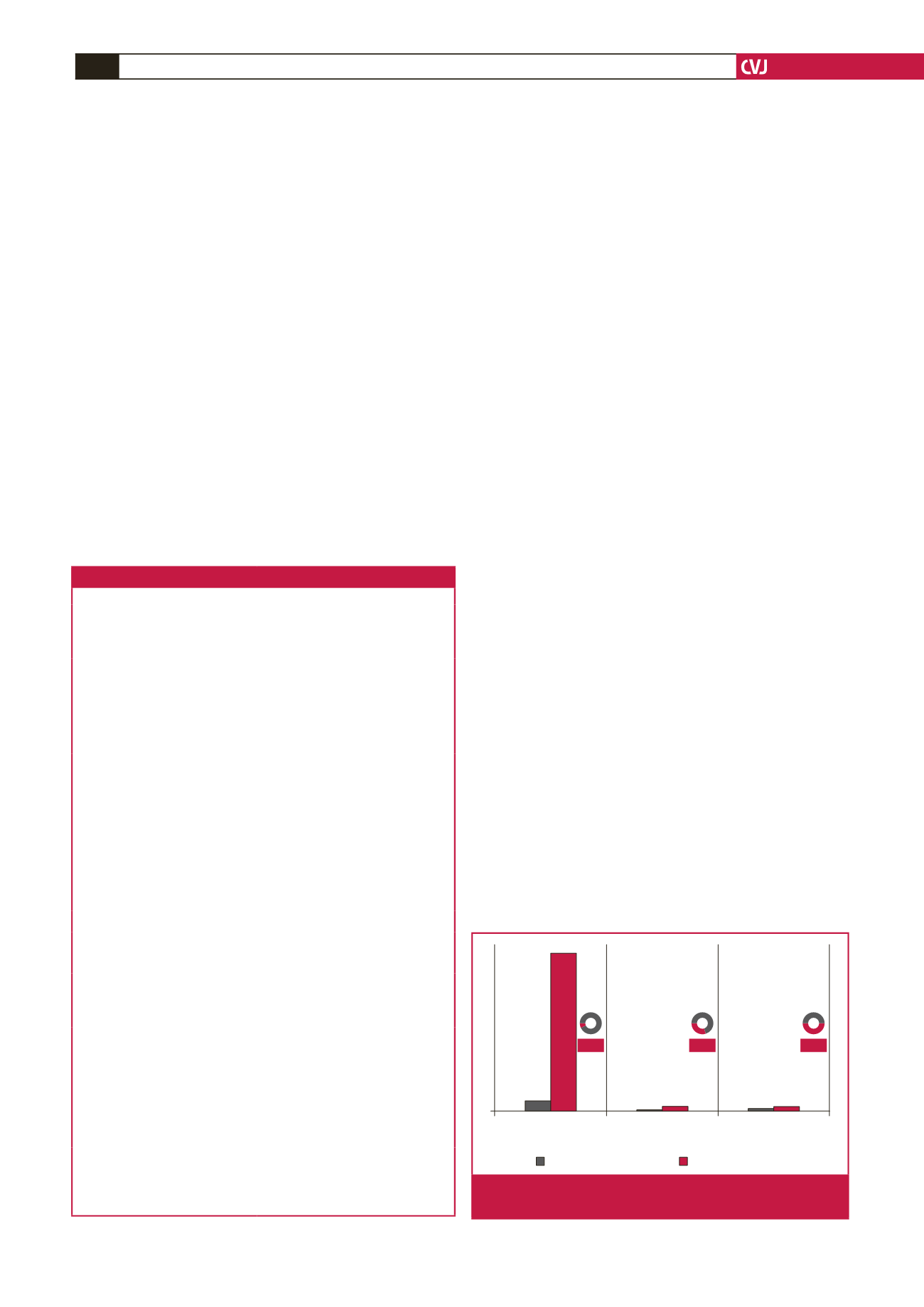
interventions in Table 2. In addition, Fig. 3 depicts the number
Table 2. Summary of the gaps identified and suggested next steps
Gaps identified
Suggested next steps
Low rates of graduates from health
professional schools due to inadequate
training posts
• Create more posts for cardiovascular
academics, promote career develop-
ment and other incentives for teaching
roles
Inadequate pool of trained cardiovas-
cular specialists
• The establishment of a private train-
ing centre for cardiologists following
the same curriculum they follow in the
state, based at a centre of excellence
Internal and external brain drain
• Close engagement of specialists in
academic hospitals and private prac-
tice
Specialists not used optimally,
considering low number of special-
ists in South Africa and therefore late
or inappropriate referral from the
community level
• Use of non-physician technicians,
medical officers in the use of hand-
held echocardiography for early
cardiac disease detection, facilitating
early referral to cardiologist/cardiotho-
racic surgeon
Specific training needs in cardiol-
ogy in pregnancy, heritable disorders
predisposing to cardiomyopathy and
arrhythmia, and metabolic disorders,
including especially familial hypercho-
lesterolaemia
• Training of obstetricians in the detec-
tion of cardiac disease, facilitating
early referral to cardiologist/cardiotho-
racic surgeon.
• Registrar rotation through special
clinics
Health system weaknesses in CVD area
Lack of strategies for increased
specialist training for cardiovascular
disease in South Africa
• Closer engagement with Departments
of Health and Education to increase
training posts
Insufficient epidemiological data on
CVD and its medical and surgical
management in South Africa
• Improve science and technology infra-
structure, acquiring better epidemio-
logical data on CVD as part of health
system-strengthening strategies
Overall low CVD scientific output,
making healthcare planning difficult
• Progressive increase in the percentage
of GDP allocated to research and
development, better recognition of
the role of the clinician–scientist and
subsequent increase in scientific output
related to cardiac disease
Health policy decision makers and
cardiovascular specialist inertia to
increase training opportunities
• Invest in regulation that promotes
public–private partnerships on
research
Low investment in research and devel-
opment infrastructure and lack of
science and technology culture
• Facilitate translational research
• Facilitate training in cardiovascular
research in South Africa and collabo-
rations with international research
entities
Adult
cardiologists
Paediatric
cardiologists
Adult
surgeons
Needed per million
Number per million
3.84
2
2
0.6
1.03
55.7
6.8%
30%
50%
Fig. 3.
Registered specialists in South Africa versus number
of specialists needed per million population.