
















 68 / 102
68 / 102

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 3, May/June 2016
190
AFRICA
Cardiology training in South Africa is not keeping
up with demand
What has changed in the training of cardiologists in the past
decade? In South Africa, cardiology training is a three year
subspecialist degree following the four-year training as a general
physician (after being a house officer and having completed the
community service time, bringing the total number of years for
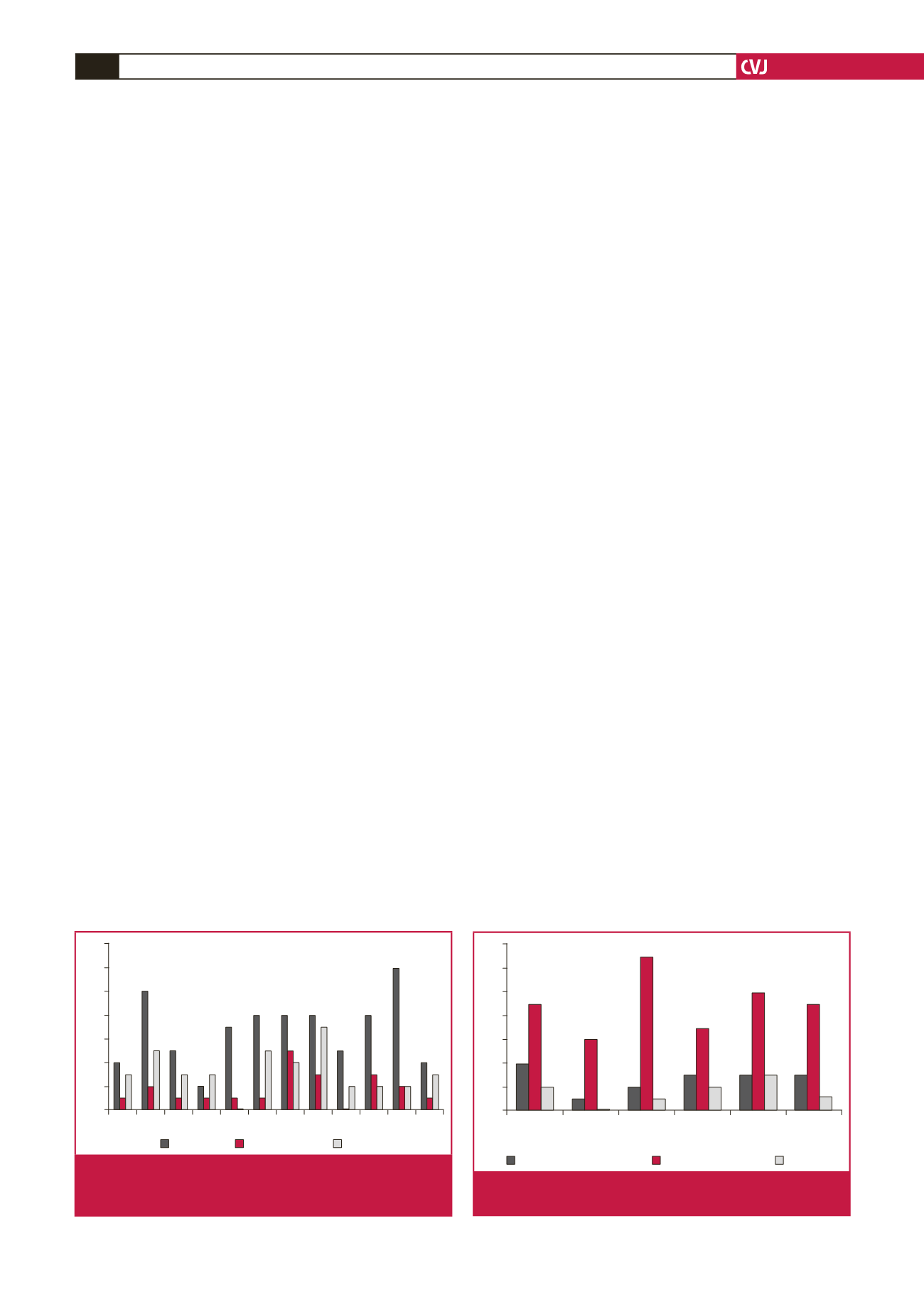
training to 15 years). Fig. 1 highlights cardiologists successfully
qualified per annum with minimal change over the last decade
and, therefore,
a de facto
decline per capita.
The number of registered cardiologists in the country is
currently about 200 for 52 million South Africans (one for
260 000). How does that compare with, for example, Brazil or
one of the other BRICs countries with similar cardiovascular
health issues to South Africa? Brazil has 8 000 board-certified
specialists in cardiology for a population of 185 million (1:23 000)
or 10 times more cardiologists and, even with that number, is not
adequately equipped for the enormous cardiovascular challenges.
17
If we use a conservative estimate based on the Brazilian
numbers, we still require at least 2 000 cardiologists in this country.
Furthermore, there is an unequal distribution of South African
cardiologists servicing the private sector, as opposed to those
servicing the public sector, where the greatest need for service
delivery exists. In order to equalise or rectify this discrepancy,
there needs to be ongoing political involvement in creating posts in
the public service sector and equalisation of remuneration.
This has a number of serious consequences. There are
inadequate or even no services at many tertiary and regional
hospitals, as well as no pacing facilities in several provinces
in the government set up. This is clearly linked to untimely
death due to easily treatable medical conditions – patients may
succumb from heart block without insertion of a pacemaker,
have inadequate therapy without reperfusion with thrombolytic
agents in acute ST-elevation myocardial infarction or suffer
inadequate management of acute heart failure. Rheumatic
heart disease is not diagnosed timeously due to poor access
to advanced diagnostic facilities, such as echocardiography
practiced by a cardiologist.
Paediatric cardiology training in South Africa
The story of congenital heart disease is one of the major
successes of medicine in the last 50 years, with the vast majority
of congenital lesions now being amenable to surgery.
18
However,
the situation in SSA is startlingly different.
19
There are only
a handful of specialised cardiothoracic centres in SSA, and
the majority of children requiring congenital heart surgery
do not have access to these centres.
20
Furthermore, cardiac
catheterisation laboratories that are able to perform procedures
such as ductal closures, pulmonary valvotomies and mitral
valvuloplasties on children are also limited in SSA.
In South Africa, we appear fortunate in that we have the
expertise to manage almost all of the congenital lesions, with the
training institutions for surgeons and cardiologists consistently
preforming over 300 cases in certain centres and over 1 500 per
year in the country. However, the reality on the ground is that,
as our primary healthcare services improve and awareness of
congenital lesions increase, more patients will be referred with
congenital heart disease requiring intervention. Despite many
medical advances in the field, we remain critically understaffed,
with increasing waiting lists and inadequate numbers of
operations per year for our population.
21,22
It is estimated that one paediatric cardiologist is required
for every 500 000 population. If we use a conservative estimate
based on half that number (one per million), we still require
at least an additional 10 paediatric cardiologists in the public
service in this country. Audits performed in 2010 and 2013
revealed that the number of paediatric cardiologists in the public
service has increased by only one since 2010. In addition, as
there is no subspecialist training for paediatric cardiothoracic
surgeons, no significant increase had occurred in the number of
children being operated on each year (Fig. 2).
Only two of the six national units consistently do over 150
operations per year. This has resulted in waiting lists in all the
public service centres that exceed 100 patients, with many dying
while waiting for surgery.
A particular concern is the fact that several provinces do
not have any regular paediatric cardiac services. This implies
that referrals between provinces are the only option for these
patients, which involves significant logistical, economic and
transport difficulties. We know that certain critical congenital
heart disease (CCHD) lesions are rarely seen in these provinces,
suggesting early demise of those affected, without a definitive
cardiac diagnosis.
The importance of paediatric cardiology training is not
only for tertiary institutions but also to increase awareness
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
14
12
10
8
6
4
2
0
Paediatric
Adult
Surgical
Fig. 1.
Number of cardiologists, paediatric cardiologists
and cardiothoracic surgeons qualified in South Africa
between 2003 and 2014.
Western
Cape
Eastern
Cape
Durban Bloem-
fontein
Chris Hani
Complex
Pretoria
Academic
14
12
10
8
6
4
2
0
Total posts required
Paediatric cardiologists
Surgeons
Fig. 2.
Consultant paediatric cardiology and cardiac surgery
staff in the Public Service.