
















 59 / 76
59 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 1, January/February 2017
AFRICA
57
adequate paediatric cardiac services.
9
The proportion is smaller
than the 24/88 (27%) reported paediatric cardiologists serving a
population of 44 million in South Africa, or one to 1.8 million
people, which is also considered inadequate.
10
The number of surgeons recorded in the present study is
also far lower than the recommended number of at least two
surgeons per centre. The reasons for the lower proportion of
paediatric cardiologists per total number of children in Nigeria
include poor training facilities in the country, such that residents
intending to do paediatric cardiology or cardiothoracic surgery
have part or all of their training in centres outside the country.
Such residents may be unwilling to return to the country to
pursue a career with the prospect of poor or lack of equipment
and materials to work with. Furthermore, not many doctors
may be interested in pursuing a career in cardiology and cardiac
surgery because of the long duration of training and the
ill-equipped training facilities.
The deficiency of manpower is further underscored by the
fact that some of these few available personnel were also visiting
physicians and surgeons to other centres, particularly private
ones. This not only highlights the need to train more personnel,
but in the opinion of the study group, also could point to
inability of the private centres to provide adequate remuneration,
tenured appointments and job security. This is against the norm
in other countries where private hospital services are able to
attract personnel from state-owned hospitals.
This is not surprising, given the capital-intensive nature of
cardiac surgery, coupled with its non-inclusion in the National
Health Insurance Scheme.
11
The private centres are therefore
unable to generate enough income to pay highly skilled full-time
staff, especially as they must rely on intermittent surgical missions
to be able to generate adequate numbers of paying patients on
whom to operate. These highly skilled staff therefore remain
in government employment, providing low levels of cardiology
Sokoto
Zamfara
Kebbi
Niger
Kwara
Oyo
Ogun
Katsina
Plateau
Borno
Taraba
Kogi
Imo
Yobe
Gombe
Adamawa
Abuja
Benue
Akwa
Ibom
Rivers
Lagos
Osun Ekiti
Ondo
Edo
Delta
Bayelsa
Cross
River
Kano
Jigawa
Bauchi
Kaduna
Nasarawa
Anambra
Enugu
Abia
Ebonyi
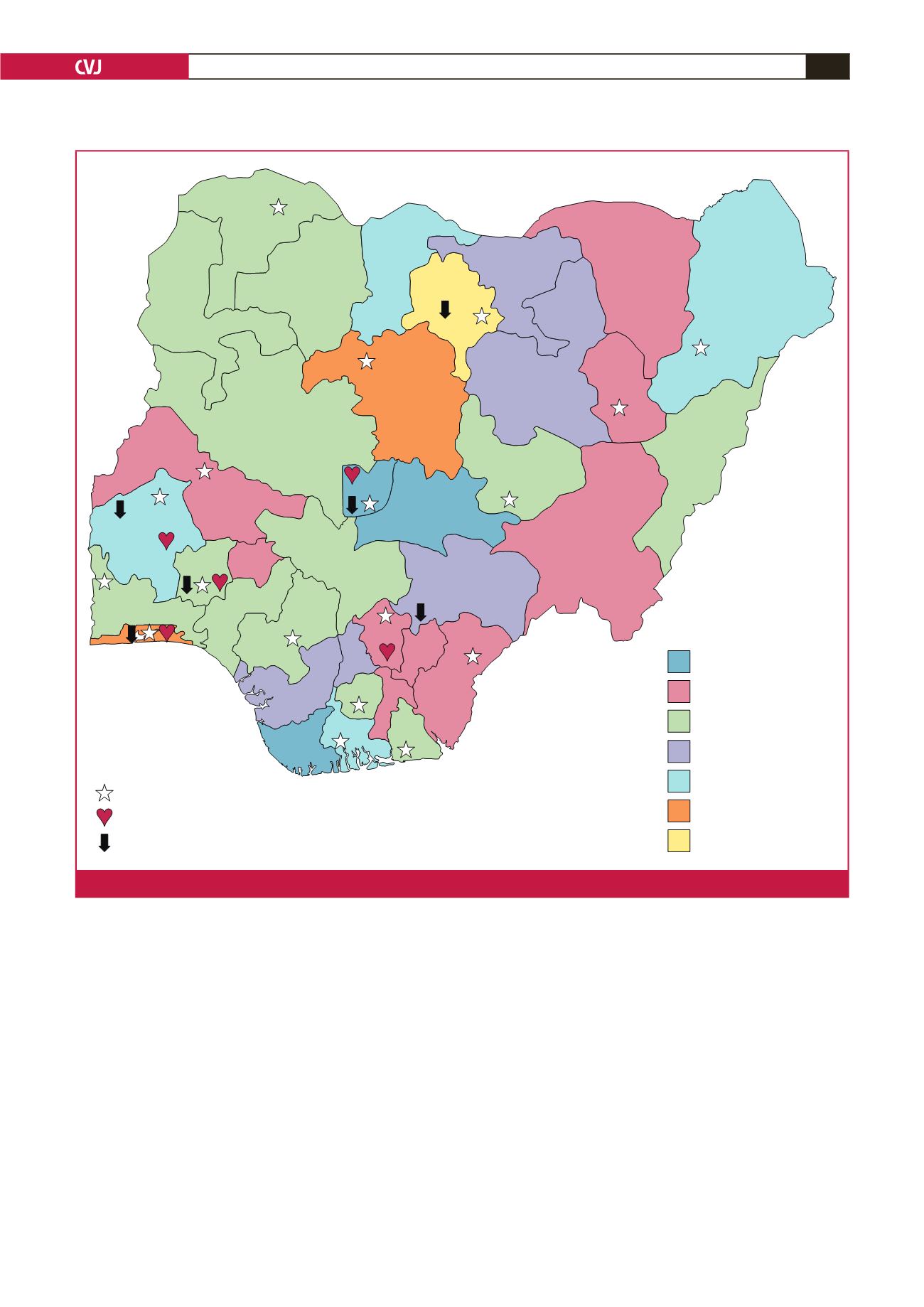
Less than 2 000 000
2 000 000 to 2 999 999
3 000 000 to 3 999 999
4 000 000 to 4 999 999
5 000 000 to 5 999 999
6 000 000 to 7 116 987
7 116 987 and more
Echocardiography availability
Open heart surgery
Cardiac catheterisation lab availability
Fig. 2.
Population map of states with echocardiography, cardiac catheterisation and open-heart surgery facilities.