
















 64 / 76
64 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 2, March/April 2017
130
AFRICA
Mora and co-workers determined the mechanisms of the
reduced risk of CHD associated with exercise in women.
2
They
found that a reduction in inflammatory biomarkers were the
largest contributors to lowered risk. These were followed, in
order, by blood pressure, lipid levels, body mass index (BMI)
and haemoglobin level. In the study, the combination of different
individual risk factors quantified only 35.5% of the total risk
reduction due to physical exercise on CHD.
2
It is therefore clear that the risk factors used by Mora and
co-workers, in terms of serological biomarkers, did not fully
quantify the risks associated with CHD. In their study, LDL,
HDL and Apo B serum levels were recorded to monitor lipid
levels, but only hsCRP serum levels were used for deducing
inflammatory levels.
2
It may therefore be possible that with the
addition of the other biomarkers indicated in Fig. 3, the effect of
moderate exercise may be better quantified.
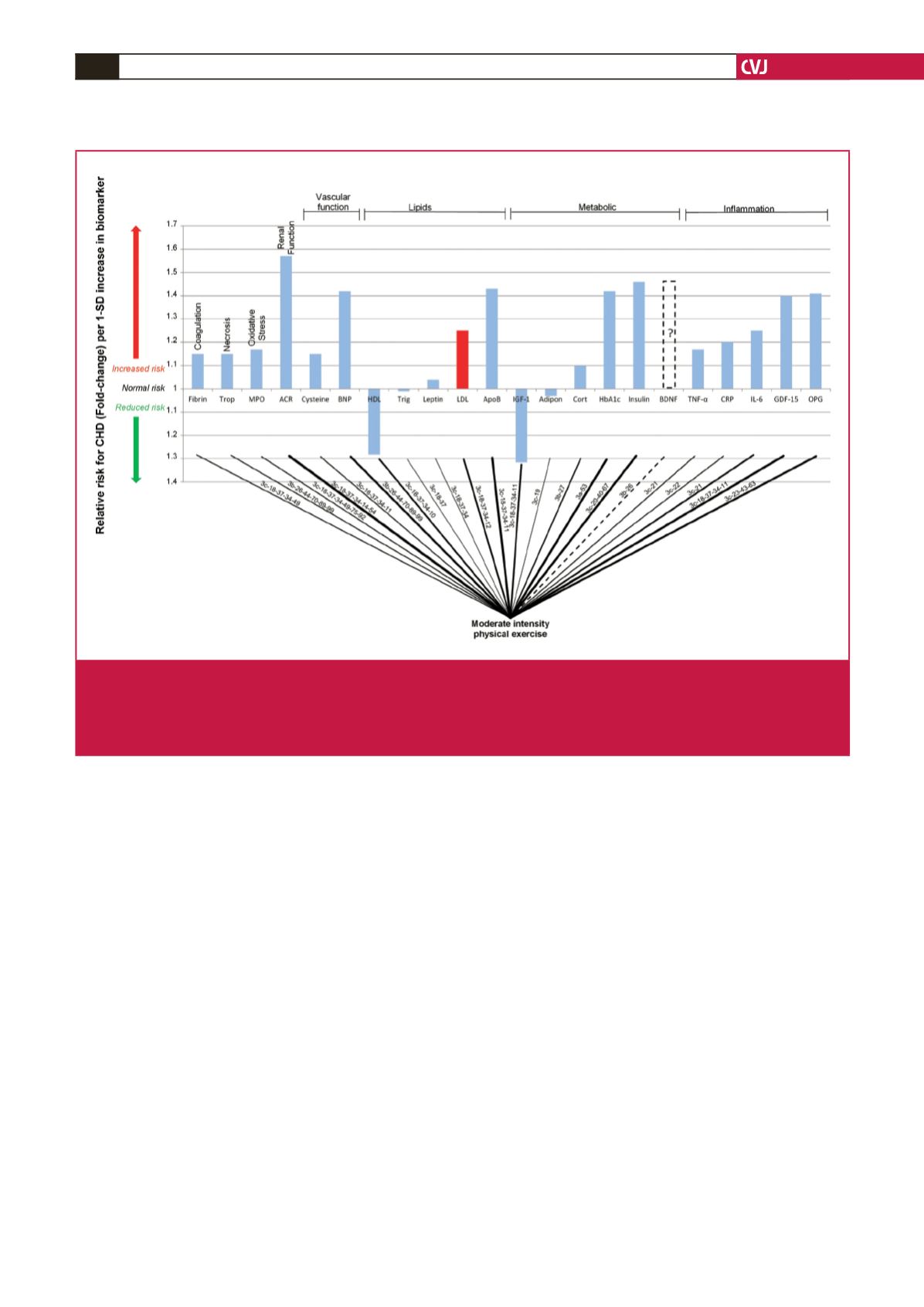
In Fig. 3, it is clear from the risk associated with inflammation
that reduction in inflammation would prove beneficial to CHD
risk. The full extent of the relationship between exercise and
inflammation has not been determined but it has been proven
that chronic moderate exercise has a systemic anti-inflammatory
effect.
5,16,32
It has further been shown that the anti-inflammatory
effect of exercise provides the largest individual risk-reduction
component of moderate exercise in women.
2
Naturally there is a strong link to the metabolic process that
is manifested in the connection to the metabolic biomarkers,
specifically insulin resistance and glycated haemoglobin level.
33,34
This connection may be largely mediated by the increased
expenditure of energy, which produces favourable effects on
CHD pathogenesis.
10,
23
Moderate exercise is also related to
changes in lipid factors such as increases in HDL cholesterol and
decreases in LDL cholesterol and Apo B levels.
33,34
Discussion
It is clear that there are a wide variety of effects of exercise on
the pathogenesis of CHD, which can be described by the changes
in biomarkers. However, from the connection graph in Fig. 3,
it is not immediately clear what the overall effect of moderate
exercise is on CHD. This effect has been quantified in the RR
reduction for CHD, which is observed in those who engage in
moderate exercise.
Moderate-intensity physical exercise of 1 100 kcal/week is
associated with an average RR of 0.75 (0.71–0.79), based on a
large meta-analysis.
35
The RR of 0.75 would correlate to a RR
reduction of 1.33-fold using the method previously described in
the Methods section.
The data from Fig. 3 show that inflammation and metabolic
Fig. 3.
Interconnection of relative risk effects of moderate exercise and serological biomarkers for CHD. ACR, albumin-to-creatinine
ratio; Adipo, adiponectin; Apo B, apolipoprotein-B; BDNF, brain-derived neurotrophic factor; BNP, B-type natriuretic peptide; Cort,
cortisol; CRP, C-reactive protein; cysteine, homocysteine; fibrin, fibrinogen; GDF-15, growth-differentiation factor-15; HbA
1c
, glyco-
sylated haemoglobin A
1
c; HDL, high-density lipoprotein; IGF-1, insulin-like growth factor-1; IL-6, interleukin-6; LDL, low-density
lipoprotein; MPO, myeloperoxidase; OPG, osteoprotegerin; TNF-
α
, tumour necrosis factor-
α
; Trigl, triglycerides; Trop, troponins.