
















 17 / 84
17 / 84

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 2, March/April 2018
AFRICA
79
The prevalence of hypercholesterolaemia (5.3% among
participants 25 and 64 years old) in this study was lower than
that found in a previous study in Luanda among an older urban
population.
15
However, this value falls within a wide range of
values from several STEPS surveys measuring the prevalence
of total cholesterol, from 2.1% in Mozambique to 26.0% in
Tanzania.
25,26
This prevalence may also be tied to the ageing
population and changes in dietary habits that most African
countries are currently facing.
28
There is a lack of solid knowledge
regarding the prevalence levels of hypercholesterolaemia in
Africa, mainly owing to the difficulties in determining values of
blood cholesterol in African communities because of the high
cost of laboratory tests. This situation presents a challenge when
comparing research results.
As described in other studies worldwide, the clustering of risk
factors helps to explain the known impacts of age, education
and obesity on the occurrence of hypertension, diabetes and
hypercholesterolaemia. The prevalence of these three conditions
was higher among individuals with less education, and increased
with age and BMI.
Obesity represents a major concern as a risk factor for
CVD and NCDs in general, and is connected with the current
nutritional transition in Africa, with a shift in the composition
and structure of diets traditionally low in fat and high in
unrefined carbohydrates toward higher intakes of refined
carbohydrates, added sugars, fats and animal-source foods.
28
This
shift may have had an impact on the rise in incidence of diabetes
over the past decades, revealed in recent literature reviews,
29-31
as
well as a WHO estimation of the rise in median prevalence of
elevated total cholesterol for this region.
2
Similar to this nutritional transition, the process of
urbanisation underway in the region must be taken into
consideration for future interventions. Living in an urban area
has been associated with a two-fold increase in the prevalence of
diabetes among this population, as described in other studies.
1,29-31
Information regarding the awareness, treatment and control
rates for the three conditions investigated is scarce for the
African continent, except for hypertension; there are also some
available data with regard to diabetes. Our findings for awareness
of hypertension were higher than those calculated in 2010 for
Africa, with an estimated 33.7% pooled awareness rate.
32
Current
values for awareness, treatment and control of hypertension are
higher than in 2011 in the same population; results for awareness
were 21.6% (95% CI: 17.0–26.9) in 2011 and 48.5% in the present
study. Values for participants who were aware of their condition
and on pharmacological treatment (13.9%, 95% CI: 5.9–29.1)
increased to 32.5%; approximately one-third of participants
were controlled in 2011 and more than half were controlled in
our study. This may have resulted from the positive effect of
identification of hypertensive individuals and medical follow up
after the first survey in 2011.
Nonetheless, the levels of awareness about hypertensive status
are still low, a situation common in Africa,
33
with levels much
lower than those in North America and Europe.
34
A similar
framework exists for diabetes awareness in Africa, with fewer
than 50% of participants in one study aware of their condition.
29
No data were found for awareness of total cholesterol levels.
The lack of primary healthcare facilities in this region,
especially in rural areas, makes the low levels of previous
measurements plausible. Furthermore, the current training of
Angolan health professionals and the availability of clinical
equipment are still focused on infectious diseases, not considering
CVD a priority. Therefore initiatives promoting the awareness
of CVD are lacking in the region, and proper monitoring of
patients’ conditions does not occur.
Moreover, the information available to the population is
not enough to convince patients to take lifelong medication in
order to treat a condition, which is usually asymptomatic. Only
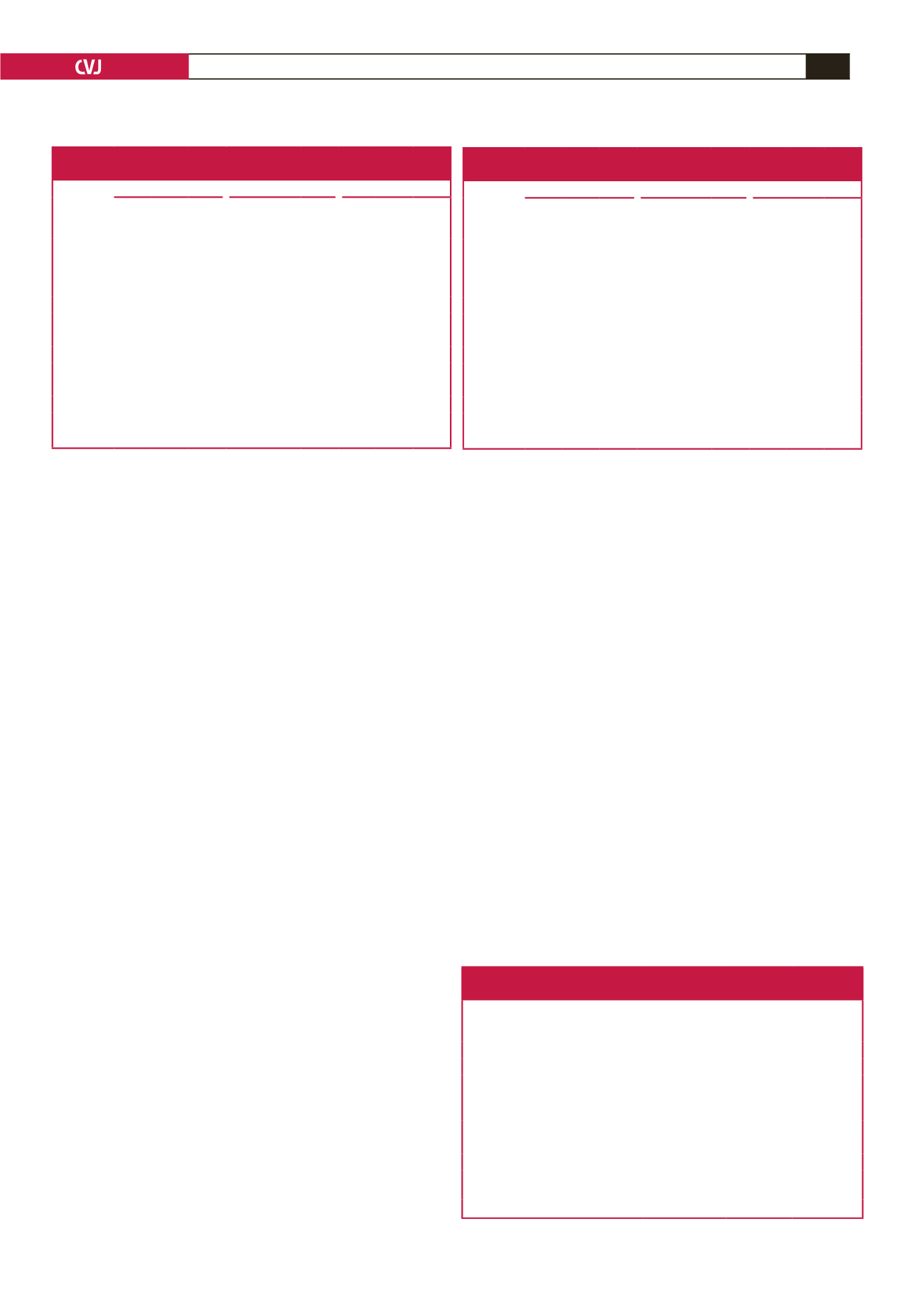
Table 9. Non-pharmacological advice by health professionals
to aware participants (Caxito, 2016)
Hypertension
(
n
=
209)
Diabetes
(
n
=
24)
Hypercholes-
terolaemia
(
n
=
3)
Advice
% (95% CI) % (95% CI)* % (95% CI)*
Reduce salt in your diet
78.5 (72.4–83.5)
100.0
100.0
Reduce fat in your diet
61.7 (55.0–68.0)
91.7
66.7
Eat at least five servings of fruit and/
or vegetables each day
58.4 (51.6–64.8)
70.8
66.7
Reduce or stop alchool consumption 51.2 (44.5–57.9)
83.3
33.3
Start or do more physical activity
34.4 (28.3–41.1)
75.0
66.7
Quit using tobacco or don’t start
31.1 (25.2–37.7)
45.8
0
Maintain a healthy body weight or
lose weight
30.1 (24.3-36.7)
75.0
66.7
*Due to the small sample size, the 95% CI was not determined.
Table 7. Awareness, treatment and control rates of diabetes by gender
(Caxito, 2016)
Awareness
Treatment
Control
All
(
n
=
24)
%
Female
(
n
=
10)
%
Male
(
n
=
14)
%
All
(
n
=
10)
%
Female
(n
=
6)
%
Male
(
n
=
4)
%
All
(
n
=
6)
%
Female
(n
=
5)
%
Male
(
n
=
1)
%
Education
(years
completed)
None
12.5 30.0 0.0 20.0 33.3 0 16.7 20.0 0
1–4
4.2 10.0 0.0 10.0 16.7 0 16.7 20.0 0
5–9
33.3 30.0 35.7 50.0 33.3 75.0 50.0 40.0 100.0
> 10
50.0 30.0 64.3 20.0 16.7 25.5 16.7 20.0 0
Age (years)
15–24
8.3 20.0 0.0 20.0 33.3 0 33.3 40.0 0
25–34
12.5 10.0 14.3 10.0 16.7 0 16.7 20.0 0
35–44
20.8 10.0 28.6 20.0 16.7 25.5 16.7 20.0 0
45–54
25.0 20.0 28.6 10.0 16.7 0
0
0
0
55–64
33.3 40.0 28.6 40.0 16.7 75.0 33.3 20.0 100.0
Table 8. Awareness, treatment and control rates of
hypercholesterolemia by gender (Caxito, 2016)
Awareness
Treatment
Control
All
(
n
=
3)
%
Female
(
n
=
2)
%
Male
(
n
=
1)
%
All
(
n
=
1)
%
Female
(
n
=
1)
%
Male
(
n
=
0)
%
All
(
n
=
1)
%
Female
(
n
=
1)
%
Male
(
n
=
0)
%
Education
(years
completed)
None
0
0
0
0
0
0
0
0
0
1–4
33.3 50.0 0
0
0
0
0
0
0
5–9
0
0
0
0
0
0
0
0
0
> 10
66.6 50.0 100.0 100.0 100.0 0 100.0 100.0 0
Age (years)
15–24
0
0
0
0
0
0
0
0
0
25–34
0
0
0
0
0
0
0
0
0
35–44
33.3 50.0 0 100.0 100.0 0 100.0 100.0 0
45–54
66.6 50.0 100.0 0
0
0
0
0
0
55–64
0
0
0
0
0
0
0
0
0