
















 66 / 76
66 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 3, May/June 2018
196
AFRICA
morphology. Also, there is no pattern to the irregularity of the
RR intervals. Based on these findings, the diagnosis of atrial
fibrillation was made.
The patient’s heart failure therapy was optimised with
diuretics. She was initially treated with a rate-control strategy and
oral anticoagulation in accordance with standard international
guidelines.
1,2
She will be seen in the rhythm clinic for consideration
of a cardioversion and a future rhythm-control strategy with
catheter ablation.
Causes of irregular, narrow-complex tachycardia
The differential diagnosis of an irregular, narrow-complex
tachycardia includes atrial fibrillation, atrial flutter with variable
atrio-ventricular (AV) block and multifocal atrial tachycardia.
Table 1 shows the differentiating electrocardiographic features.
Atrial fibrillation (AF) is the most common cause of an
irregular, narrow-complex tachycardia, affecting approximately
33 million people worldwide.
3
Patients of older age are at
increased risk of developing AF, as well as patients with
hypertensive, valvular and ischaemic heart disease.
4
AF can be
triggered by acute alcohol intoxication, thyrotoxicosis, sepsis or
dehydration.
5
More recently, AF has been shown to be associated
with obesity and obstructive sleep apnoea.
6-8
In atrial fibrillation there is chaotic, asynchronous atrial
impulse propagation, with multiple wavelets that course
irregularly through the atria and reach the AV node at irregular
intervals, which cause irregular AV nodal conduction. On the
ECG (Fig. 3), atrial fibrillation is recognised by an irregular
RR interval with no pattern to the irregularity and the absence
of distinct P waves. Very rapid, continuous, irregular ‘chaotic’
activity (called fibrillatory waves) can be seen. These are best
seen in V1 and can be coarse or fine. Fibrillatory waves can be as
fast as 400–600 per minute. The ventricular rate, however, can be
fast, normal or slow, depending on AV nodal conduction.
9
Atrial flutter (AFL), the second most common pathological
supraventricular tachyarrhythmia, shares many risk factors with
atrial fibrillation.
10
In contrast to AF, AFL is caused by rapid,
continuous atrial activity around a fixed re-entry circuit, usually
an anti-clockwise circuit in the right atrium. Flutter waves have
a saw-tooth pattern and are best appreciated in standard lead
II and lead V1 (Fig. 4). It can be difficult to differentiate atrial
flutter with variable block from coarse atrial fibrillation.
In contrast to AF, flutter waves are regular and discrete,
uniform in morphology (in keeping with the organised re-entry
circuit) with a fixed atrial rate usually around 300 per minute
(can range between 240 and 360). The ventricular rate depends
on the degree of AV block (e.g. QRS rate of approximately 150
Table 1. Diagnostic approach to irregular, narrow-complex tachycardia
Key features
Atrial fibrillation
Atrial flutter
Multifocal atrial tachycardia
Atrial wave morphology Fibrillatory waves (f waves, irregular in
morphology and amplitude)
Flutter waves
(F waves, regular in morphology and amplitude)
At least three different P-wave morpholo-
gies in same lead
Atrial wave timing
Variable
Identical
Variable
Atrial wave cycle length 400–600 per min
240–360 per min
Usually < 130 per min
PR interval
No obvious PR interval
No obvious PR interval
Variable PR intervals
Ventricular (QRS)
response
Usually narrow QRS complexes, often vary in
amplitude, constantly irregular RR intervals
Usually narrow QRS complexes, constant F/R
ratios
Usually narrow QRS complexes, random
and constantly irregular RR intervals
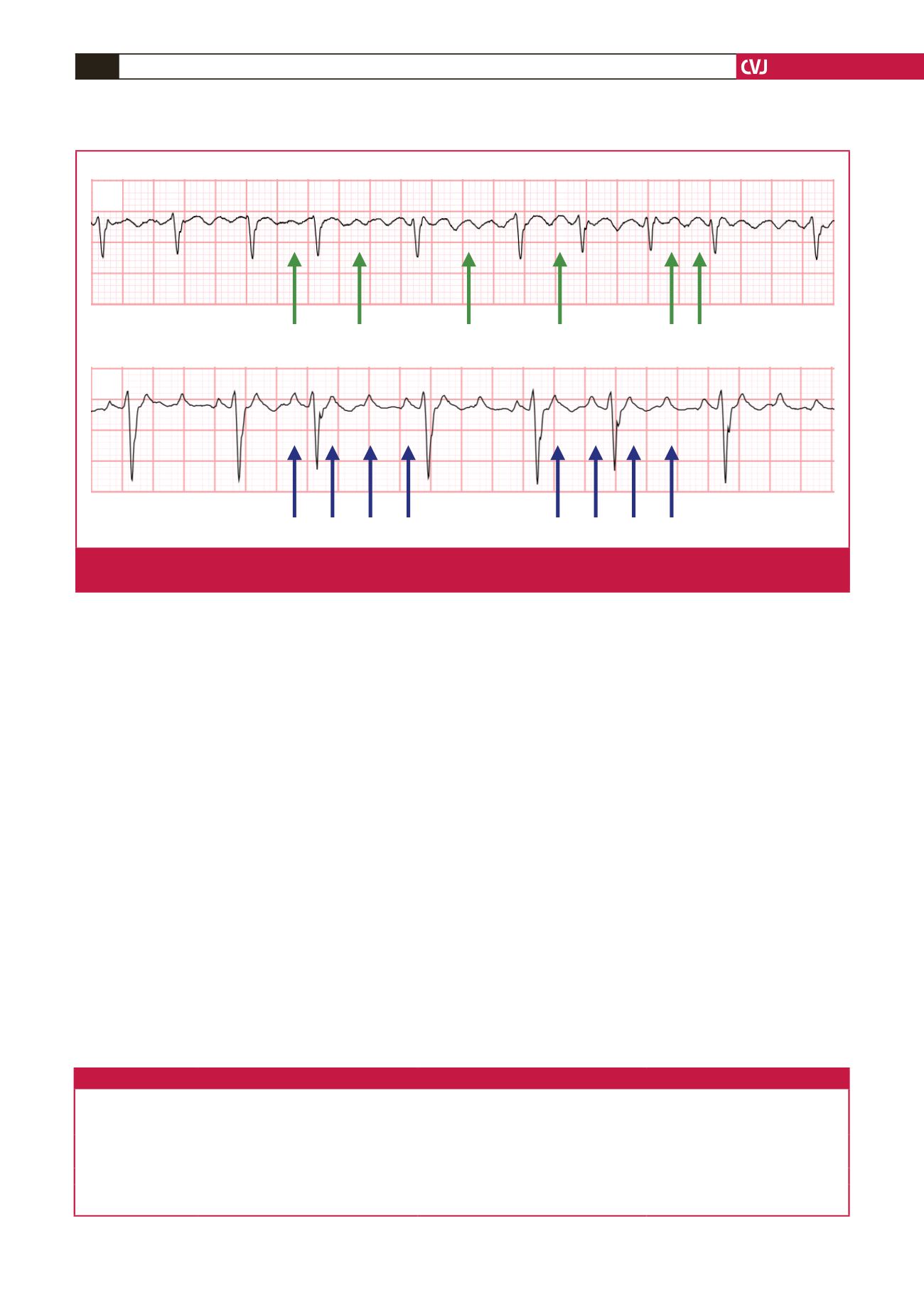
V1
Atrial fibrillation
Atrial flutter with a variable block
Note fibrillatory waves have constantly changing morphologies
Note flutter waves have an identical morphology throughout
V1
V1
Atrial fibrillation
Atrial flutter with a variable block
Note fibrillatory waves have constantly changing morphologies
Note flutter waves have an identical morphology throughout
V1
Atrial fibrillation
Atrial flutter with a variable block
Note fibrillatory waves have constantly changing morphologies
Note flutter waves have an identical morphology throughout
Fig. 2.
Comparison of coarse atrial fibrillation (fibrillatory wave morphology is not regular and uniform) and atrial flutter (flutter-wave
morphology is regular and uniform).