
















 7 / 76
7 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 3, May/June 2018
AFRICA
137
mitral regurgitation had greater LV dimensions and greater LV
mass, though overall LV systolic function was not different.
Procollagen IC peptide (PIP) and procollagen III N-terminal
pro-peptide (PIIINP) were similar between patients and controls,
however, matrix metalloproteinase-1 (MMP-1) activity was
increased in the patient group. The authors concluded that
chronic rheumatic mitral regurgitation is characterised by the
predominance of collagen degradation rather than increased
synthesis and myocardial fibrosis.
RHD is characterised by chronic inflammation which, in
many other inflammatory cardiac conditions,
6,8-10
is associated
with frequent focal myocardial fibrosis. In this small study,
the authors reported the incidence of myocardial fibrosis on
LGE-CMR at 18%. It would have been instructive if the
investigators had utilised native T1 mapping or ECV to assess
for the presence of diffuse myocardial fibrosis in RHD, which
in my experience is found commonly. The authors attribute
the infrequent LGE to increased expression of biomarkers
of collagen degradation. However, the relationship of serum
biomarkers of collagen synthesis, which have low specificity for
cardiac fibrosis, has been inconsistently reported in the literature,
with a prior publication reporting increased biomarkers of
collagen synthesis in RHD.
19
In the future, CMR may play an increasingly important and
complementary role to echocardiography in the evaluation and
management of patients with RHD. An advantage of CMR
over echocardiography in RHD is the ability to provide accurate
and reproducible information on tissue characteristics, including
• Anatomy
• Function (global and regional)
• Vascular assessment (PWV, distensibility)
• Tissue characterisation (inflammation, oedema)
• Myocardial deformation (strain)
• Rest and stress perfusion (inducible ischaemia)
• Viability
• Regional fibrosis
• Diffuse fibrosis
• Flow/4-D flow
• Myocardial energetics
• Myocardial lipidosis
Fig. 2.
Multiparametric capability of CMR.
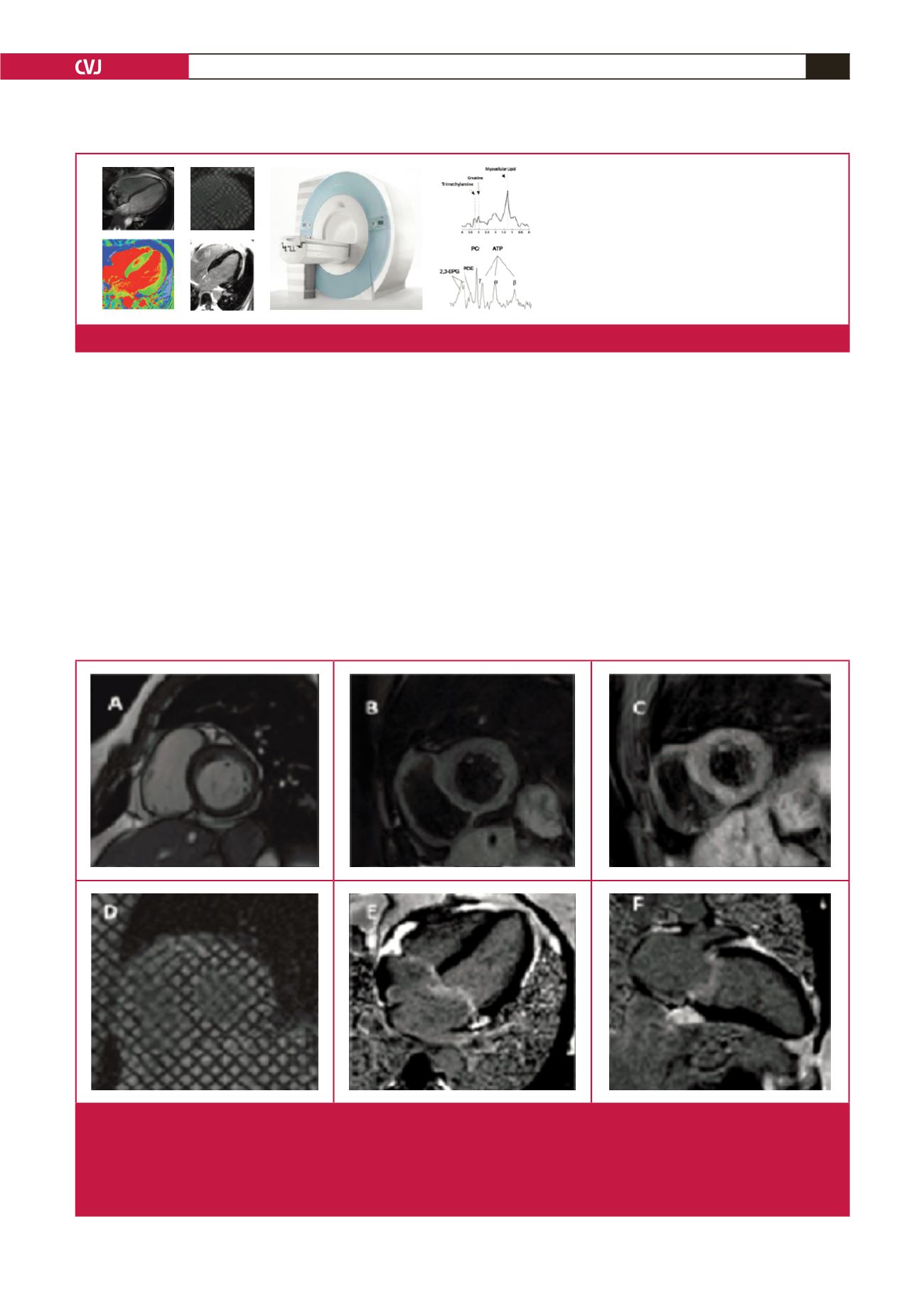
Fig. 3.
Patient with heart block and acute myocarditis confirmed to be due to acute rheumatic fever. A. balanced steady-state free-
precession image showing a short-axis ciné; B. T1-weighted image showing increased myocardial signal-intensity ratio; C.
T2-weighted imaging showing increased myocardial signal-intensity ratio (in keeping with myocardial oedema); D. Ciné
tagging imaging of the short axis confirming impaired circumferential strain and strain rate; E. Horizontal long-axis (four-
chamber) LGE image showing no myocardial enhancement but evidence of valvulitis, with valvular and atrial enhancement;
F. Vertical long-axis (two-chamber) LGE image confirming lack of myocardial LGE, but mitral valve enhancement.