


















 60 / 66
60 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 32, No 3, May/June 2021
170
AFRICA
Since the standard treatment of CP is pericardiectomy,
fibrotic and calcified pericardium should be removed to the
extent of enhancing the efficacy of treatment. Furthermore,
calcified pericardium effectively grows into the cardiac surface,
thereby increasing the risk of heart injury when attempting to
remove the pericardium.
The complications of pericardiectomy are as follows:
bleeding due to myocardial injury, coronary artery injury
and phrenic nerve injury, therefore, when conducting a
pericardiectomy, an ultrasonic scalpel should be used due to
its safety and compatibility with minor tissue damage.
4
Total
pericardiectomy is defined as radical phrenic-to-phrenic excision
of the pericardium, from the great arteries superiorly to the
diaphragmatic surface inferiorly,
5
and in case of fibrotic and
calcified pericardium, total pericardiectomy is advisable to
prevent future exacerbation. Although good surgical outcome
of left anterolateral thoracotomy for recurrent CP has been
reported in a previous study, total pericardiectomy using this
approach is difficult and the article does not mention total
pericardiectomy.
6
Recurrence or exacerbation of CP following previous partial
pericardiectomy is common. Interestingly, a previous report
described a case involving re-pericardiectomy 43 years after a
previous pericardiectomy had been performed.
7
The authors
of that report indicated that the cause of CP recurrence was
the inadequate removal of calcified pericardium. Therefore,
inadequate pericardiectomy renders the early surgical results
unfavourable and increases the risk of recurrent CP.
The patient in our case had undergone prior pericardiectomy
to treat only anterior calcified pericardium. However, during
postoperative follow up, heart failure occurred due to the
recurrence of CP two years later. Furthermore, the calcified
pericardium had changed over time; however, a haematoma was
found to have developed prior to the second operation, which
contributed to the development of the atypical calcification. As
a result, the enveloped haematoma occupied the space between
the heart and the diaphragm. We conclude that the calcified
tissue not only perturbed diastolic function, but also physically
compressed the heart.
Conclusion
It is important to remove as much fibrotic and calcified
pericardium as possible since effective pericardiectomy
contributes to improved early surgical results and prevents the
recurrence of CP. Inadequate pericardiectomy can result in an
unfavourable postoperative course and prognosis; therefore, total
pericardiectomy should be performed for CP.
We thank Editage
(www.editage.jp) for English language editing.
References
1.
Biçer M, Özdemir B, Kan
İ
, Yüksel A, Tok M,
Ş
enkaya I. Long-term
outcomes of pericardiectomy for constrictive pericarditis.
J Cardiothorac
Surg
2015;
10
: 177.
2.
Chowdhury UK, Subramaniam GK, Kumar AS, Airan B, Singh R,
Talwar S,
et al.
Pericardiectomy for constrictive pericarditis: a clinical,
echocardiographic, and hemodynamic evaluation of two surgical tech-
niques.
Ann Thorac Surg
2006;
2
: 522–529.
3.
Ling LH, Oh JK, Schaff HV, Danielson GK, Mahoney DW, Seward
JB,
et al
. Constrictive pericarditis in the modern era: evolving clinical
spectrum and impact on outcome after pericardiectomy
. Circulation
1999;
100
: 1380–1386.
4.
Uchida T, Bando K, Minatoya K, Sasako Y, Kobayashi J, Kitamura S.
Pericardiectomy for constrictive pericarditis using the harmonic scalpel.
Ann Thorac Surg
2001;
3
: 924–925.
5.
Vistarini N, Chen C, Mazine A, Bouchard D, Hebert Y, Carrier M,
et
al
. Pericardiectomy for constrictive pericarditis: 20 years of experience at
the Montreal Heart Institute.
Ann Thorac Surg
2015;
1
: 107–113.
6.
Yunfei L, Tao L, Yongjun Q. Re-pericardiectomy for recurrent chronic
constrictive pericarditis: left anterolateral thoracotomy is a better
approach
. J Cardiothorac Surg
2019;
1
: 152.
7.
Madershahian N, Franke U, Bruhin R, Wahlers T. Reoperation for
calcific constrictive pericarditis 43 years after pericardiectomy.
J Card
Surg
2005;
6
: 549–551.
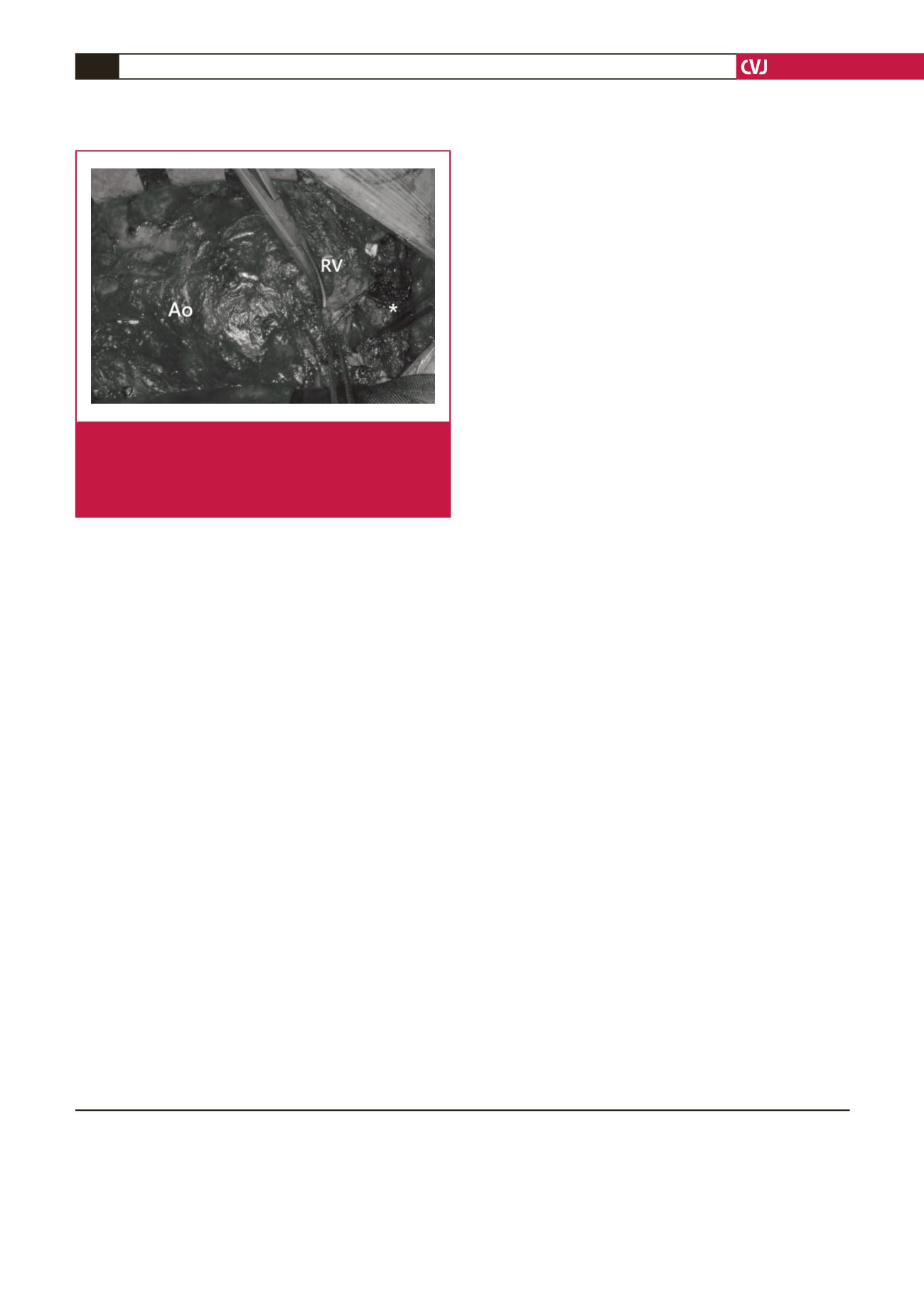
Fig. 3.
The calcified pericardium strongly fixed on the heart
surface is gently removed from the heart using an
electric knife and ultrasonic scalpel. Ao: aorta; RV:
right ventricle; *thick calcified pericardium on the infe-
rior portion of the heart.